Class 1C Antiarrhythmic Drugs are Safe in Patients with Arrhythmia-induced Cardiomyopathy Following Recovery of Left Ventricular Ejection Fraction
Abstract Body (Do not enter title and authors here): Background: Class 1C antiarrhythmic drugs (AADs), such as flecainide and propafenone, are effective first-line agents for rhythm control in atrial tachyarrhythmias. The Cardiac Arrhythmia Suppression Trial (CAST) suggested class 1C AADs increase mortality in patients with myocardial ischemia, limiting their use to those without structural heart disease. Still, the safety and efficacy of class 1C AADs in arrhythmia-induced cardiomyopathy (AiCM) following recovery of LVEF are unexplored.
Goals: To evaluate the safety and efficacy of class 1C AADs in treating atrial tachyarrhythmias in patients with AiCM following recovery of LVEF compared to patients with no prior cardiomyopathy.
Methods: We conducted a retrospective cohort study at a single academic center, including adult patients with atrial fibrillation, flutter, or tachycardia and a history of AiCM with recovered LVEF prescribed class 1C AADs since 2010. The control group included patients with atrial tachyarrhythmias prescribed class 1C AADs without prior reduced LVEF. Patients with ischemic or other structural heart diseases were excluded. Primary outcomes were all-cause mortality and sustained ventricular arrhythmias. Secondary outcomes were recurrent atrial tachyarrhythmia, need for electrical cardioversion (ECV) or ablation, and medication discontinuation. Statistical analyses used Cox proportional hazards models.
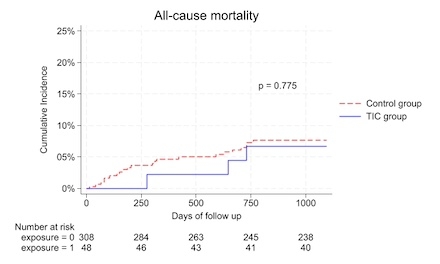
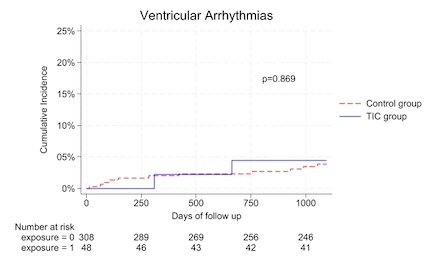
Results: Among 356 patients (308 control, 48 AiCM), no significant difference was observed in mortality (7.0% vs. 6.3%, unadjusted HR 0.84, 95% CI 0.25-2.80, p=0.822; adjusted HR (aHR) 0.90, 95% CI 0.15-5.32, p=0.906) or ventricular arrhythmias (3.6% vs. 4.2%, HR 1.14, 95% CI 0.25-5.12, p=0.838; aHR 1.36, 95% CI 0.18-10.50, p=0.767). The recurrence of atrial arrhythmia was similar between the control and AiCM groups (34.4% vs. 41.7%, p=0.328). The need for ECV and ablation, while greater in the AiCM group, was not significantly different between the groups. However, medication discontinuation was significantly higher in the AiCM group (45.8% vs. 29.9%, p=0.027), primarily due to recurrent arrhythmias and medication intolerance.
Conclusions: Class 1C AADs appear safe in patients with atrial tachyarrhythmias and AiCM following recovery of LVEF, comparable to those without prior cardiomyopathy. However, AiCM patients exhibited higher rates of medication discontinuation, indicating potential challenges in treatment adherence. Further large-scale studies are needed to confirm these findings.
Pohlkamp, Ryan
(
University of Arkansas for Medical Sciences
, Little Rock , Arkansas , United States )
Chidambaram, Vignesh
(
University of Arkansas for Medical Sciences
, Little Rock , Arkansas , United States )
Kumar, Amudha
(
Loyola University Medical Center
, Maywood , Illinois , United States )
Ghanta, Nikhila
(
University of Arkansas for Medical Sciences
, Little Rock , Arkansas , United States )
Odueke, Adetayo
(
University of Arkansas for Medical Sciences
, Little Rock , Arkansas , United States )
Vallurupalli, Srikanth
(
University of Arkansas for Medical Sciences
, Little Rock , Arkansas , United States )
Paydak, Hakan
(
UAMS/CAVHS
, Little Rock , Arkansas , United States )
Author Disclosures:
Ryan Pohlkamp:DO NOT have relevant financial relationships
| Vignesh Chidambaram:No Answer
| Amudha Kumar:No Answer
| Nikhila Ghanta:No Answer
| Adetayo Odueke:DO NOT have relevant financial relationships
| Srikanth Vallurupalli:No Answer
| Hakan Paydak:DO NOT have relevant financial relationships