Inpatient Tricuspid Valve transcather and surgical procedural outcomes: A Propensity Matched analysis
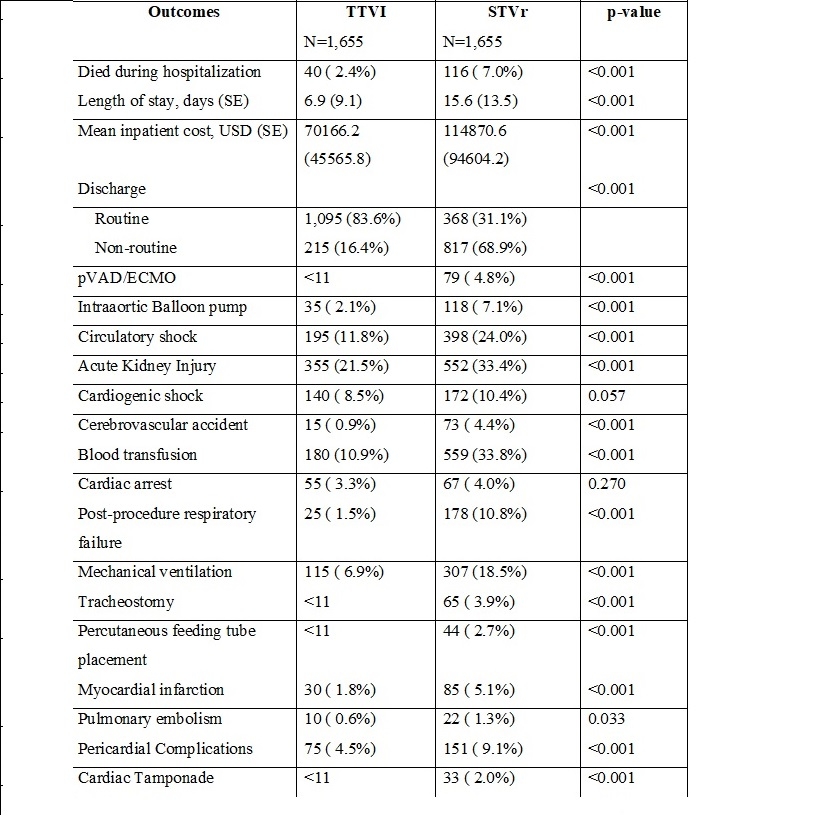
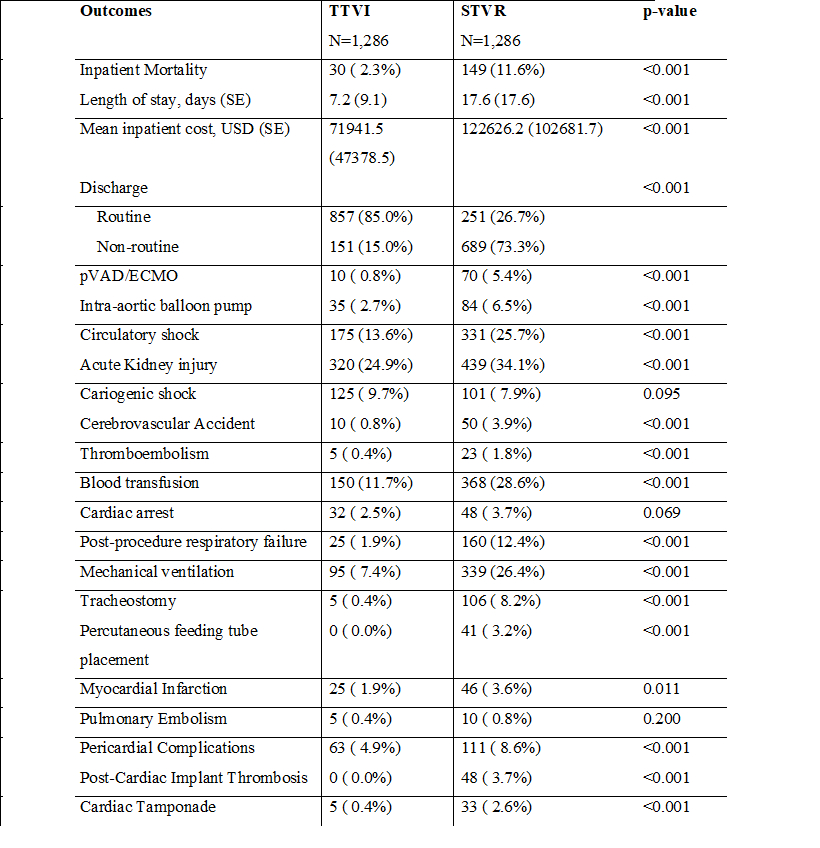
Abstract Body (Do not enter title and authors here): Background: Tricuspid regurgitation (TR) is a common valvular heart disease, and associated with increased cardiovascular mortality. Adverse events from surgical treatment of severe TR are limiting this approach. Aim: To analyze the outcomes of using surgical and transcatheter TV interventions across the United States. Methods: We used The National Inpatient Sample (NIS) data base and included data between January 1, 2011 and December 31, 2020. We selected patients who underwent Transcatheter tricuspid valve intervention (TTVI), surgical TR repair (STVr), and surgical TR replacement (STVR). TTVI patients were propensity-matched 1:1 to STVr and STVR using nearest neighbor matching. Analyses were conducted using STATA version 17. Results: Between 2011 and 2020, a total of 98,202 TV interventions were identified. Of these, 1,830 (1.9%) underwent TTVI, 76,747 (78.2%) underwent STVr and 19,625 (19.9%) underwent STVR. Patients receiving TTVI were older, more likely to be white and to be treated at a teaching hospital. STVR accounted for the highest proportion of TV procedure-related deaths overall, followed by surgical TV replacement, and lastly, TTVI. In our PSM analysis, STVr and STVR were associated with increased inpatient mortality (7% vs 2.3%, 11.6% vs 2.4%, respectively), when compared to TTVI (p<0.001). Among patients who underwent tricuspid intervention, the odds of experiencing circulatory shock were higher in STVr (24.0% vs 11.8%) and STVR (11.6% vs 2.3%) when compared to TTVI (P<0.001). Moreover, STVr (7.0% vs 2.4%) and STVR (11.6% vs 2.3%) were also associated with higher likelihood of post-procedure respiratory failure (p<0.001). Patients with STVr and STVR experienced longer hospital stays, higher inpatient costs, increased likelihood of non-routine discharge, utilization of mechanical circulatory support (MCS), cerebrovascular accidents, blood transfusions, mechanical ventilation, myocardial infarctions, and pericardial complications Conclusions: Our study does present findings favoring TTVI over surgical interventions. TTVI demonstrates advantages in terms of hemodynamic stability, inpatient mortality, length of stay, and likelihood of MCS use. Nevertheless, additional research is necessary to characterize the long-term durability of TTVI.
Alayyat, Ahmad
(
Hamilton Medical Center
, Dalton , Georgia , United States )
Alhuneafat, Laith
(
University of Minnesota
, Minneapolis , Minnesota , United States )
Rasheed, Waqas
(
Texas Tech University Health Sciences Center at Amarillo
, Amarillo , Texas , United States )
Kapcin, Kyle
(
Allegheny Health Network
, Pittsburgh , Pennsylvania , United States )
Manalo, Kathryn
(
Allegheny General Hospital
, Pittsburgh , Pennsylvania , United States )
Maaita, Abdel Latif Mohd Abdellatif
(
Istanbul Okan University
, Istanbul , Turkey )
Jabri, Ahmad
(
Henry Ford Hospital
, Detroit , Michigan , United States )
Author Disclosures:
Ahmad Alayyat:DO NOT have relevant financial relationships
| Laith Alhuneafat:DO NOT have relevant financial relationships
| Waqas Rasheed:No Answer
| Kyle Kapcin:DO NOT have relevant financial relationships
| Kathryn Manalo:DO NOT have relevant financial relationships
| Abdel latif mohd abdellatif Maaita:DO NOT have relevant financial relationships
| Ahmad jabri:No Answer