Scientific Sessions 2024
/
Sex Differences in CVD 1
/
Racial Disparities in Management and Outcomes of Acute Myocardial Infarction and Non-Acute Myocardial Infarction Related Cardiogenic Shock: An Analysis of the National Inpatient Sample Database
American Heart Association
173
0
Final ID: Su3078
Racial Disparities in Management and Outcomes of Acute Myocardial Infarction and Non-Acute Myocardial Infarction Related Cardiogenic Shock: An Analysis of the National Inpatient Sample Database
Abstract Body (Do not enter title and authors here): Background Cardiogenic shock (CS) has high morbidity and mortality rates. There is limited understanding of race differences in the management and outcomes of CS.
Methods We queried the US National Inpatient Sample database (years 2016-2021) for CS hospitalizations in adults and categorized them by presence of acute myocardial infarction (AMI) on admission. Using multivariable logistic regression modeling, we adjusted for age, sex, income, insurance, comorbidities, and prior cardiac interventions and compared racial differences in use of and time to interventions, inpatient mortality, and cardiac arrest during hospitalization for AMI-CS and non-MI-CS.
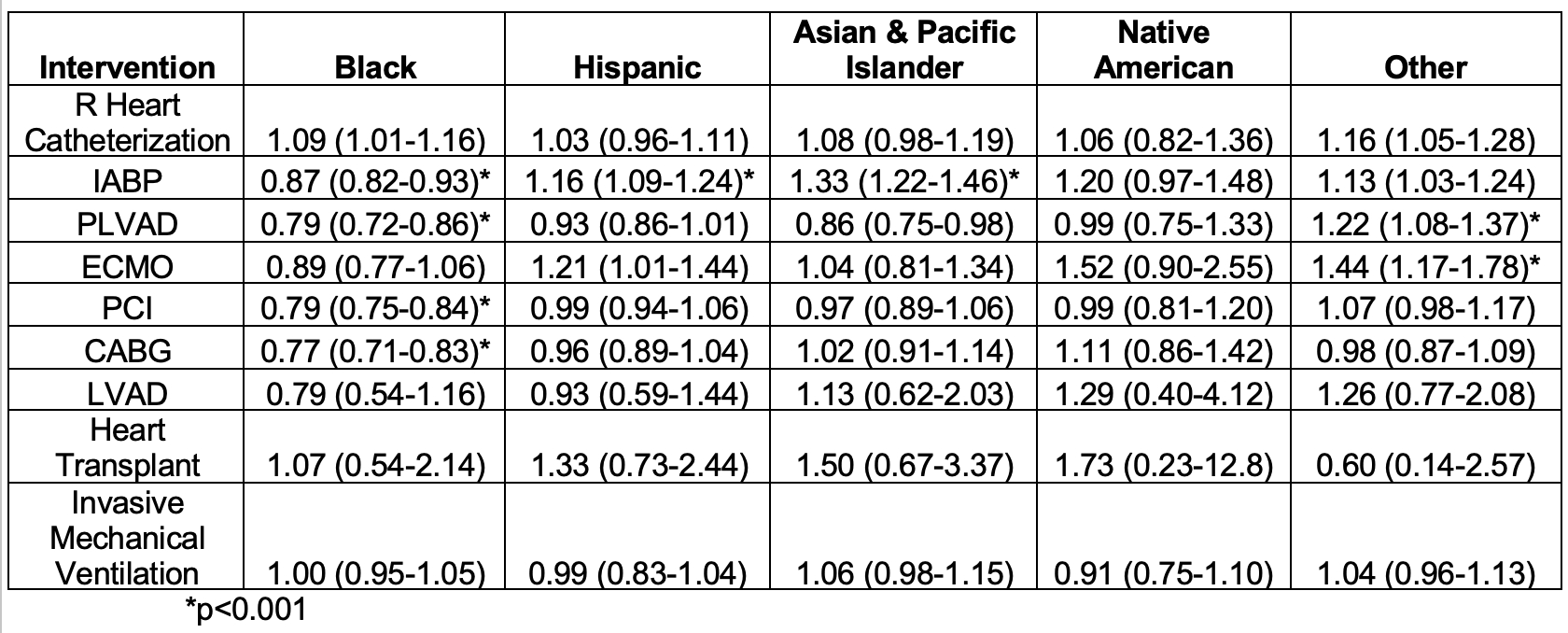
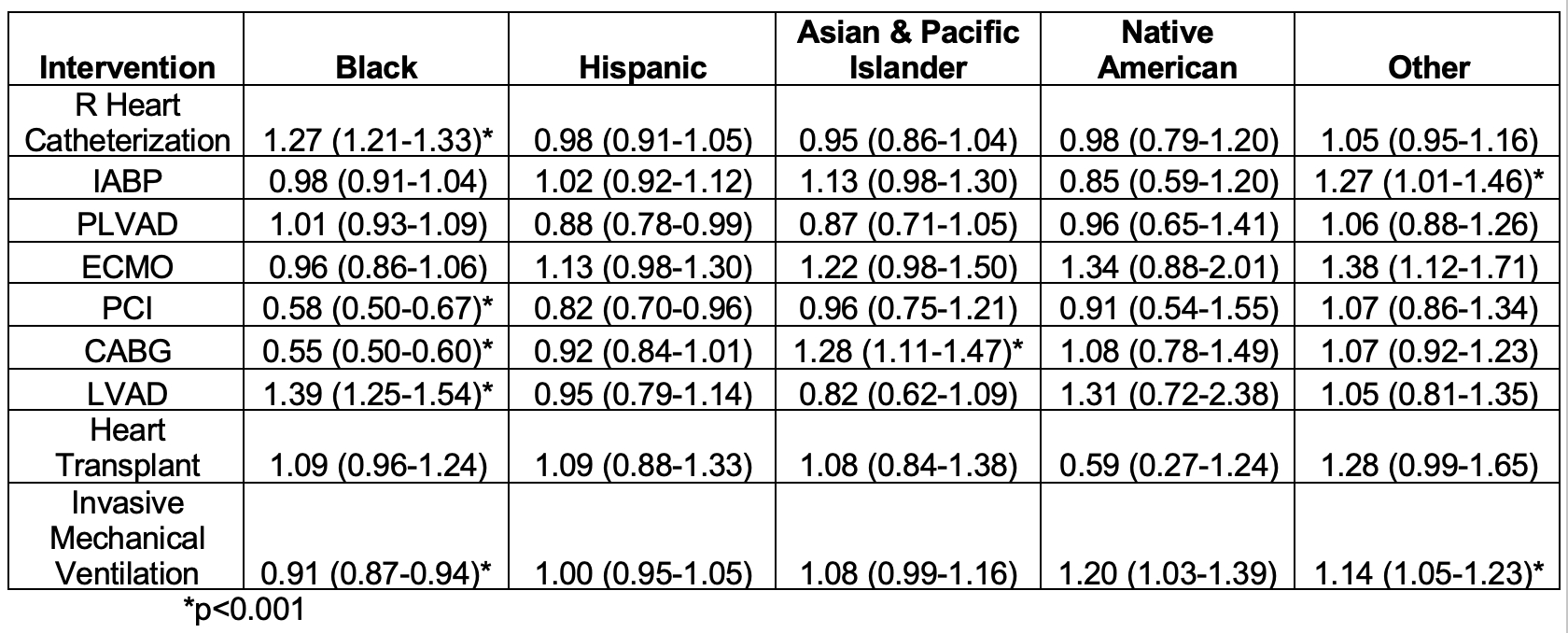
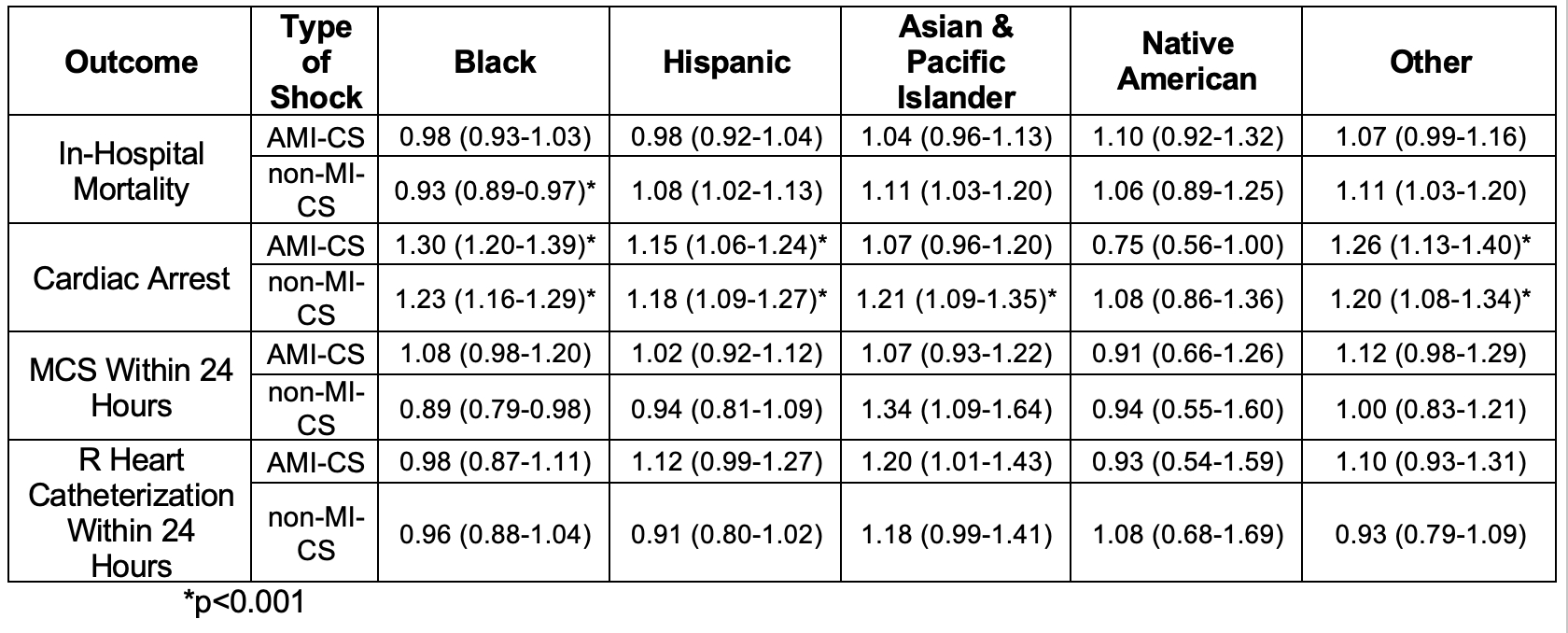
Results Out of a total 1,012,050 weighted hospitalizations for CS, 60% involved non-MI-CS, while 40% were AMI-CS. Among AMI-CS hospitalizations, Black patients were less likely to receive IABP (aOR: 0.87, 95%CI: 0.82-0.93), pLVAD (aOR: 0.79, 95%CI: 0.72-0.86), PCI (aOR: 0.79, 95%CI: 0.75-0.84), and CABG (aOR: 0.77, 95%CI: 0.71-0.83), than White patients (all p<0.001). For non-MI-CS hospitalizations, Black patients were less likely to receive PCI (aOR: 0.58, 95%CI: 0.50-0.67), CABG (aOR: 0.55, 95%CI: 0.50-0.60), and invasive mechanical ventilation (aOR: 0.91, 95%CI: 0.87-0.94) and were more likely to receive right heart catheterization (aOR: 1.27, 95%CI: 1.21-1.33) and LVAD (aOR: 1.39, 95%CI: 1.25-1.54) when compared to White patients (all p<0.001). In both types of CS, treatment of Hispanic, Asian, and Native American patients was largely comparable to that of White patients. Regardless of CS type, Black patients were more likely to have cardiac arrest during hospitalization. Race was not seen to impact likelihood of inpatient mortality or early treatment within 24 hours in either non-MI-CS or AMI-CS hospitalizations.
Conclusions Differential management of CS by race is most notable between Black and White patients with Black patients being less likely to receive most treatments. Inpatient mortality rates remain comparable across race and ethnicity groups. Future studies should further investigate the clinical impact of racial differences in management and assess survival based on time to procedure and length of stay.
Desai, Anushka
(
Georgetown University School of Medicine
, Washington , District of Columbia , United States )
Minhas, Anum
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Rahman, Faisal
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Author Disclosures:
Anushka Desai:DO NOT have relevant financial relationships
| Anum Minhas:DO NOT have relevant financial relationships
| Faisal Rahman:No Answer