Abstract Body (Do not enter title and authors here):
Background: Transcatheter aortic valve-in-valve (VIV) replacement has emerged as a valid alternative to conventional re-operation for the treatment of failed bioprosthetic surgical aortic valves. Self-expandable valves (SEV) and balloon-expandable valves (BEV) are the two major devices used. The aim of this study is to compare outcomes between SEV and BEV when used for transcatheter aortic valve replacement (TAVR) procedures in failed surgical prostheses.
Methods: A comprehensive search was conducted on PubMed, Scopus, Web of Science, Cochrane Library, and Embase databases to identify studies comparing aortic valve in valve (ViV) with SEV and BEV for failed surgical aortic prostheses from inception to May 22, 2024. To estimate the effect size, dichotomous outcomes were pooled as risk ratio (RR), and continuous outcomes were pooled as mean difference (MD) with their respective 95% confidence interval (CI).
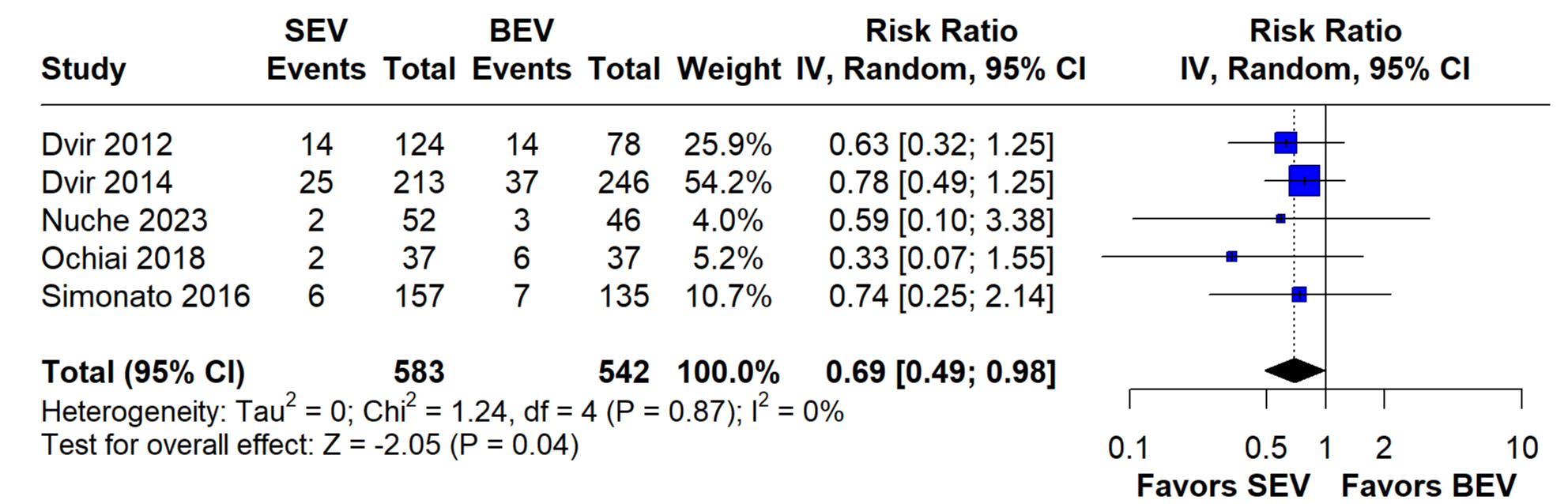
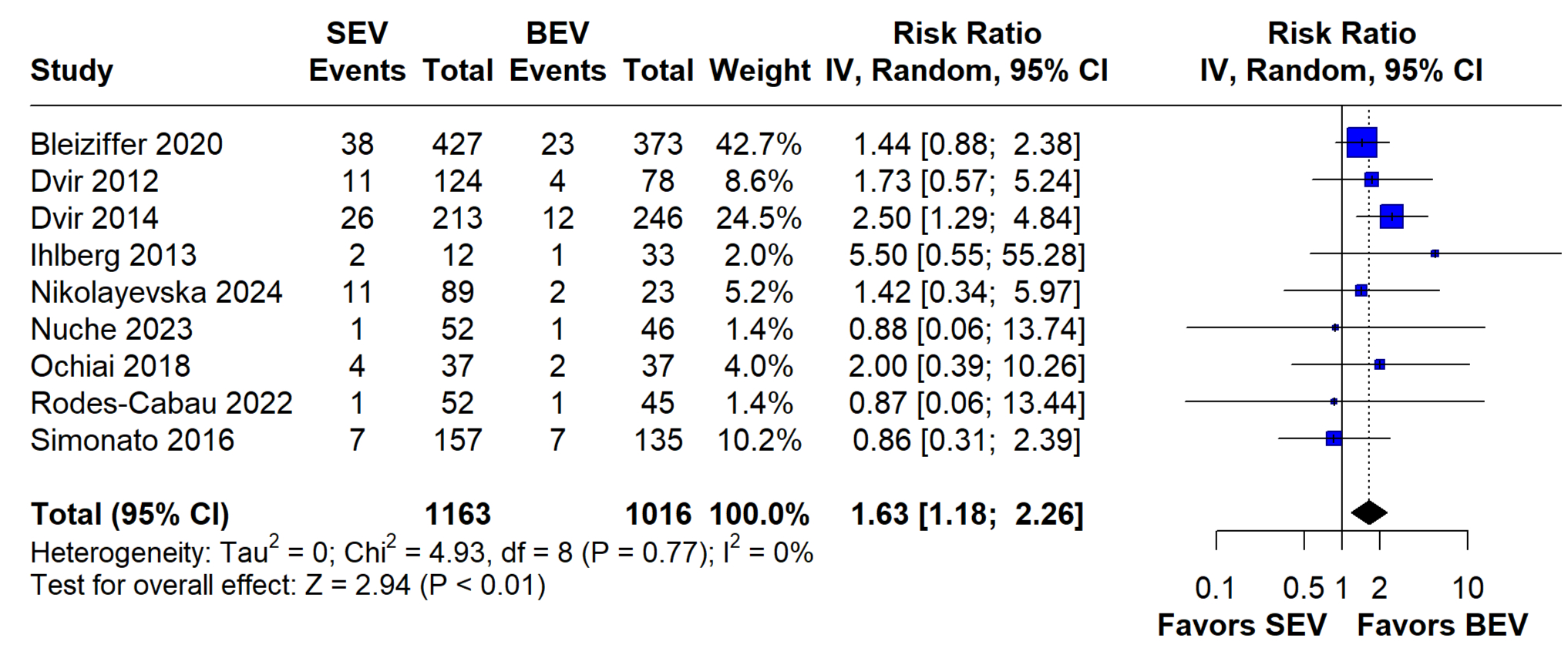
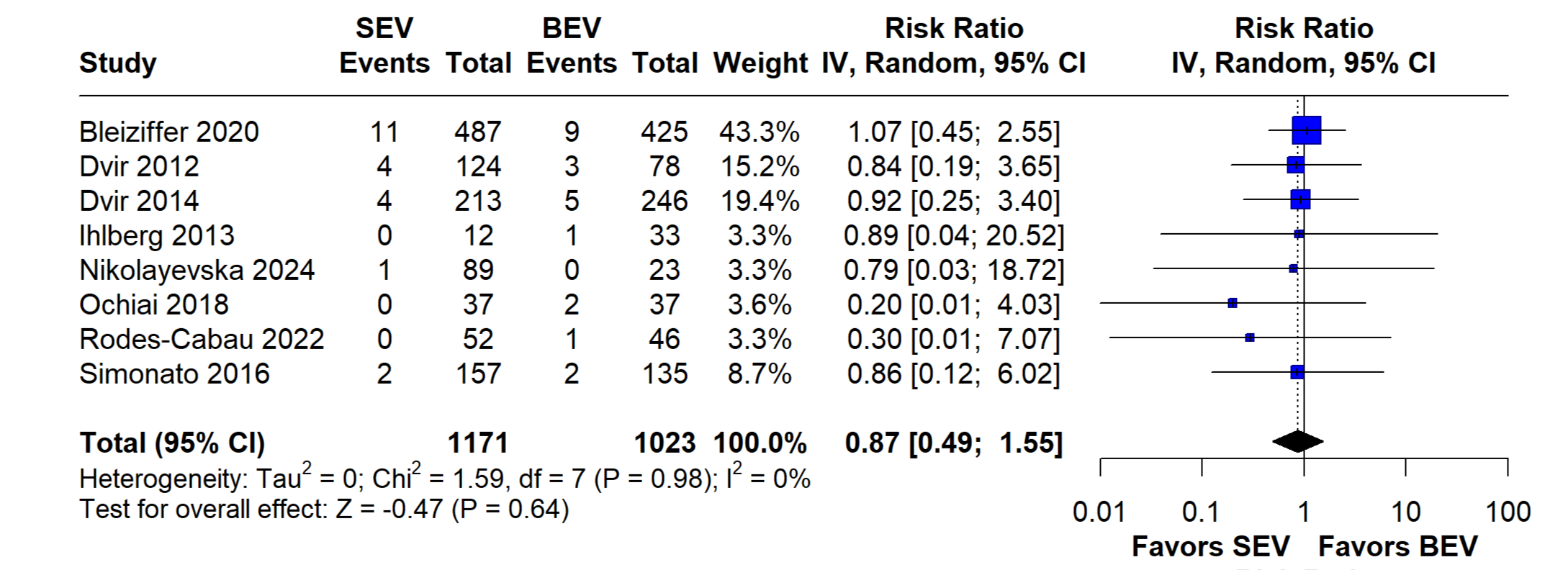
Results: We included nine studies with a total of 1258 patients in the SEV group and 1079 in the BEV group. Compared to patients in the BEV group, patients in the SEV group had significantly lower one-year mortality (RR = 0.69; 95% CI: [0.49-0.98], p = 0.04). SEV group also had less incidence of severe patient protheses mismatch (RR = 0.49; 95% CI: [0.32-0.75], p <0.01). On the other hand, patients with SEV had a significantly higher risk of moderate to severe aortic regurgitation (AR) (RR = 2.71; 95% CI: [1.69-4.36], p = <0.01) as well as permanent pacemaker implantation (PPI) (RR = 1.63; 95% CI: [1.18 - 2.26], p <0.01). There was no difference in the rate of coronary obstruction (RR = 0.87; 95% CI: [ 0.49-1.55], p = 0.64), stroke (RR = 0.82; 95% CI: [0.42-1.58], p = 0.55), and short-term mortality (RR = 0.76; 95% CI: [0.49-1.18], p = 0.23) between both groups. One-year change in mean aortic valve gradient was comparable between both groups (MD = -13.94; 95% CI:[-31.16-3.28], p = 0.11).
Conclusion: The present systematic review and meta-analysis found that for patients with failed surgical protheses who underwent transcatheter aortic VIV, SEV was associated with significantly less rate of one-year mortality and severe patients Prosthesis mismatch, but higher rates of PPI implantation and AR of moderate or higher degree. These findings provide valuable information in guiding proper selection of devices for patients with degenerated aortic surgical bioprostheses.