Cardiac Tamponade And Constrictive Effusive Pericarditis Caused By Metastatic High-Grade Follicular-Derived Thyroid Carcinoma
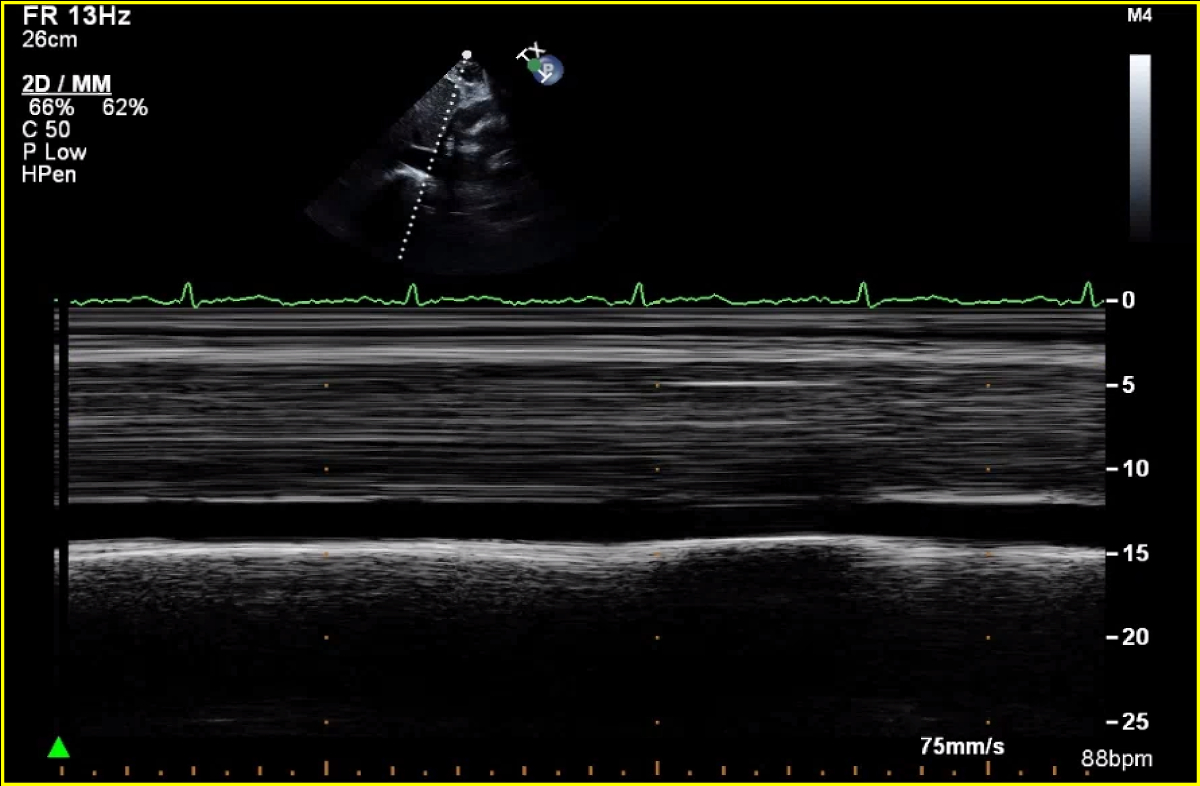
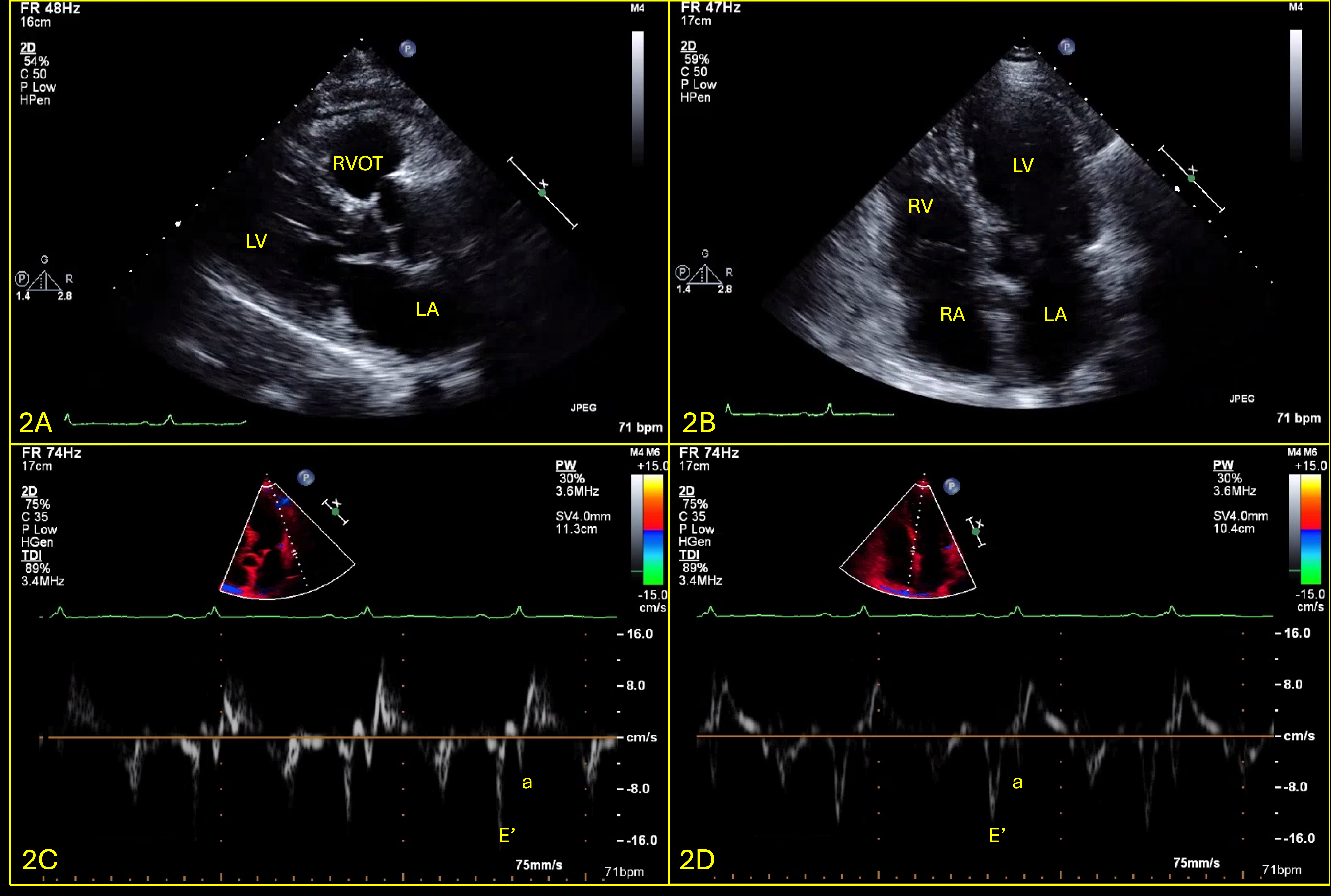
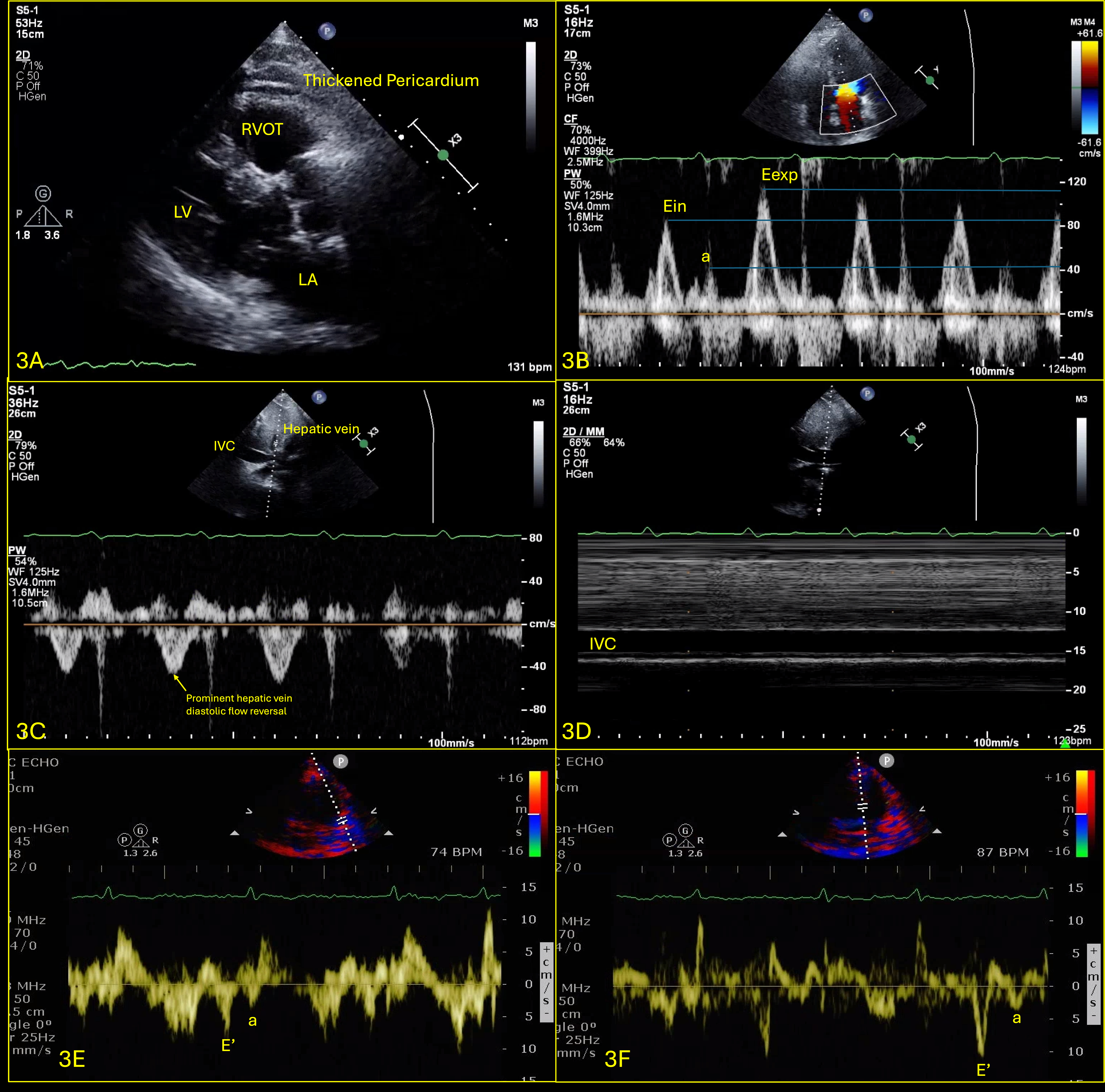
Abstract Body (Do not enter title and authors here): Case Presentation: A 76-year-old male, non-smoker, with history of HLD and NIDDM, presented with several weeks of dyspnea and cough, unresponsive to outpatient treatments. He was normotensive and found to have new onset atrial fibrillation at a rate of 110bpm and pulsus paradoxus with a difference of 15mmHg. CT chest showed a 2.2cm thyroid nodule along with a pericardial effusion (PE), confirmed to be tamponade on TTE (Fig.1). A TTE showed resolution of tamponade after the pericardial window (Fig.2). Pericardial fluid cytology was positive for malignant cells. Patient was discharged, had an outpatient PET CT which showed uptake in the thyroid, pericardial region & right supraclavicular lymph node (LN). The patient developed symptoms of heart failure, prompting his 2nd visit to the hospital after 3 weeks. A repeat TTE showed a small PE with effusive-constrictive physiology (Fig.3). He was started on high dose steroids and diuresed as tolerated, but his symptoms did not improve. He underwent thyroid nodule and right supraclavicular LN biopsy, which revealed high grade follicular thyroid carcinoma (FTC). His course was complicated by multiorgan failure, prompting transfer to another facility for pericardiectomy; during which he was found to have extensive tumor infiltration into the myocardium; he then went into shock and passed away shortly after.
Discussion: Effusive-constrictive pericarditis (ECP) is a rare clinical condition characterized by PE with constrictive physiology1. Hancock defined ECP as a pathophysiological form of cardiac compression due to a constricted visceral pericardium and PE, with the hallmark sign of persistently elevated right atrial pressure despite removal of pericardial fluid2. ECP can rarely be caused by malignancies, attributing 5% of cases2. FTC is a well-differentiated thyroid malignancy that typically metastasizes to distant sites such as the lungs and bones, but pericardial involvement is extremely rare. To date, there has been one reported case of PE caused by FTC, but the PE did not reaccumulate, possibly due to early recognition and radiation therapy3. To our best knowledge, this case report represents the first documented case of ECP caused by FTC. Our case demonstrates the complexity of diagnosing/managing it, which underscores the need for a multidisciplinary approach and comprehensive diagnostic evaluation in patients with PE, especially when associated with malignancies that rarely metastasize to the pericardium.
Achuthanandan, Supraja
(
Maimonides Medical Center
, Brooklyn , New York , United States )
Tamazyan, Vahagn
(
Maimonides Medical Center
, Brooklyn , New York , United States )
Naeem, Azka
(
Maimonides Medical Center
, Brooklyn , New York , United States )
Harutyunyan, Hakob
(
Maimonides Medical Center
, Brooklyn , New York , United States )
Munoz Martinez, Alejandro
(
Maimonides Medical Center
, Brooklyn , New York , United States )
Sadiq, Adnan
(
Maimonides Medical Center
, Brooklyn , New York , United States )
Hollander, Gerald
(
Maimonides Medical Center
, Brooklyn , New York , United States )
Author Disclosures:
Supraja Achuthanandan:DO NOT have relevant financial relationships
| Vahagn Tamazyan:DO NOT have relevant financial relationships
| Azka Naeem:DO NOT have relevant financial relationships
| Hakob Harutyunyan:DO NOT have relevant financial relationships
| Alejandro Munoz Martinez:No Answer
| Adnan Sadiq:No Answer
| Gerald Hollander:No Answer