Cardioprotective Role of Sodium-glucose cotransporter 2 Inhibitors in Cancer Patients Undergoing Anthracycline Therapy: A Systematic Review and Meta-Analysis
Abstract Body (Do not enter title and authors here): Background: Sodium-glucose cotransporter 2 inhibitors (SGLT2i) are known to have cardioprotective effects in diabetes mellitus and heart failure patients. Anthracyclines, chemotherapeutic agents used in the treatment of various malignancies, carry a high risk of cardiotoxicity and heart failure. The use of SGLT2i to prevent cardiotoxicity and adverse cardiovascular outcomes in cancer patients undergoing anthracycline therapy is not well established.
Hypothesis: This meta-analysis aims to evaluate the relationship between the use of SGLT2i for the reduction of adverse cardiovascular outcomes in patients undergoing anthracycline therapy.
Methods: We systematically searched for relevant articles published until March 2024 on PubMed, Cochrane, and Embase. The hazard ratio (HR) was pooled using the random-effects model and a p-value of <0.05 was considered statistically significant.
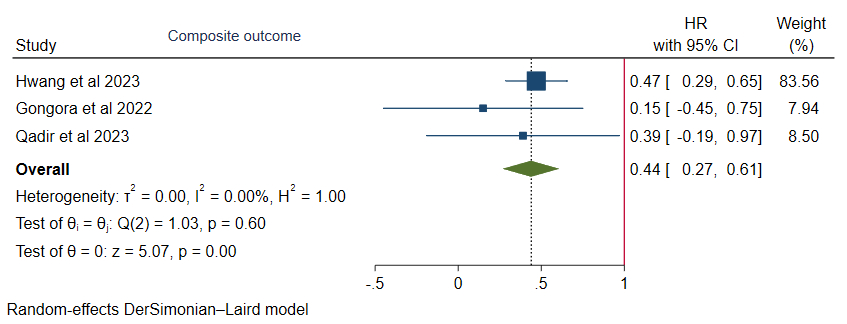
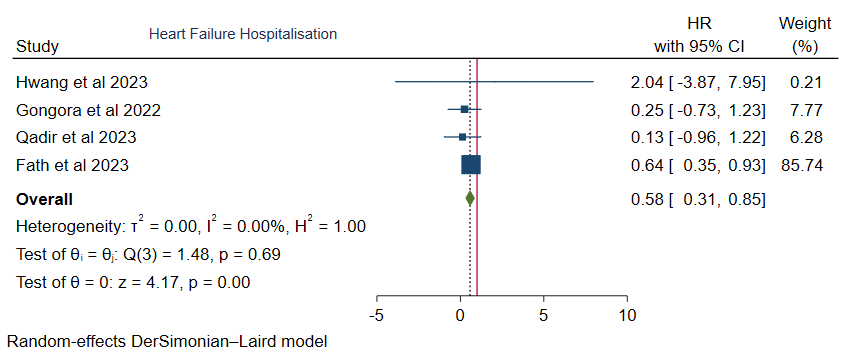
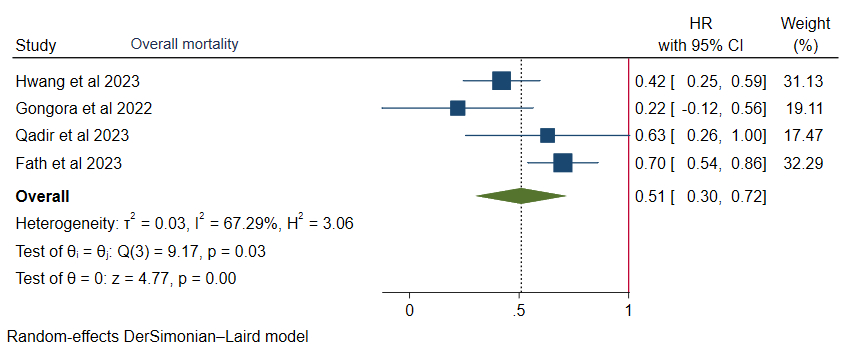
Results: Four studies involving 5590 patients (SGLT2i group: 1617 and non-SGLT2i group: 3973) were included in our analysis. The composite outcome, which included heart failure hospitalization, acute myocardial infarction, ischemic stroke, and death was significantly reduced in individuals receiving SGLT2i therapy compared to those who did not receive it (HR: 0.44, 95% CI: 0.27-0.61, I2=0.00%, p<0.005). Moreover, the risk of hospitalization due to heart failure (HR: 0.58, 95% CI: 0.31-0.85, I2=0.00%, p<0.005), and all-cause mortality (HR: 0.51, 95% CI: 0.30-0.72, I2=67.29%, p<0.005) were significantly lower among patients treated with SGLT2i. However, the risk of new heart failure diagnosis (HR: 0.65, 95% CI: 0.27-1.04, I2=0.00%, p=0.86) was comparable.
Conclusion: The findings suggest that SGLT2i among cancer patients with anthracycline therapy is associated with a lower risk of composite outcomes, heart failure hospitalization, and overall mortality.
Shrestha, Abhigan
(
Medical Research Hub, Nepal
, Kathmandu , Nepal )
Adhikari, Ashok
(
Universal College Of Medical Sciences
, Bardaghat , Nepal )
Mainali, Nischal
(
Kathmandu Medial College and Teaching Hospital
, Kathmandu , Nepal )
Shrestha, Sajina
(
Kist medical college and teaching hospital
, Lalitpur , Nepal )
Khandait, Harshwardhan
(
Trinitas Regional Medical Center
, Elizabeth , New Jersey , United States )
Shrestha, Aayush
(
B.P. Koirala Institute of Health Sciences
, Gorkha , Nepal )
Khadka, Sulochana
(
UPMC
, Pennsylvania , Pennsylvania , United States )
Jaiswal, Vikash
(
JCCR Cardiology Research
, Jaunpur , India )
Author Disclosures:
Abhigan Shrestha:DO NOT have relevant financial relationships
| Ashok Adhikari:DO NOT have relevant financial relationships
| Nischal Mainali:DO NOT have relevant financial relationships
| Sajina Shrestha:No Answer
| Harshwardhan Khandait:DO NOT have relevant financial relationships
| Aayush Shrestha:DO NOT have relevant financial relationships
| Sulochana Khadka:DO NOT have relevant financial relationships
| Vikash Jaiswal:DO NOT have relevant financial relationships
Jiang Chao, Dong Jianzeng, Cai Jun, Anderson Craig, Du Xin, Tang Yangyang, Han Rong, Song Yanna, Wang Chi, Lin Xiaolei, Yi Yang, Rodgers Anthony, Ma Changsheng