A Risk Prediction Score for Shockable Sudden Cardiac Arrest: Validation in the Framingham Heart Study
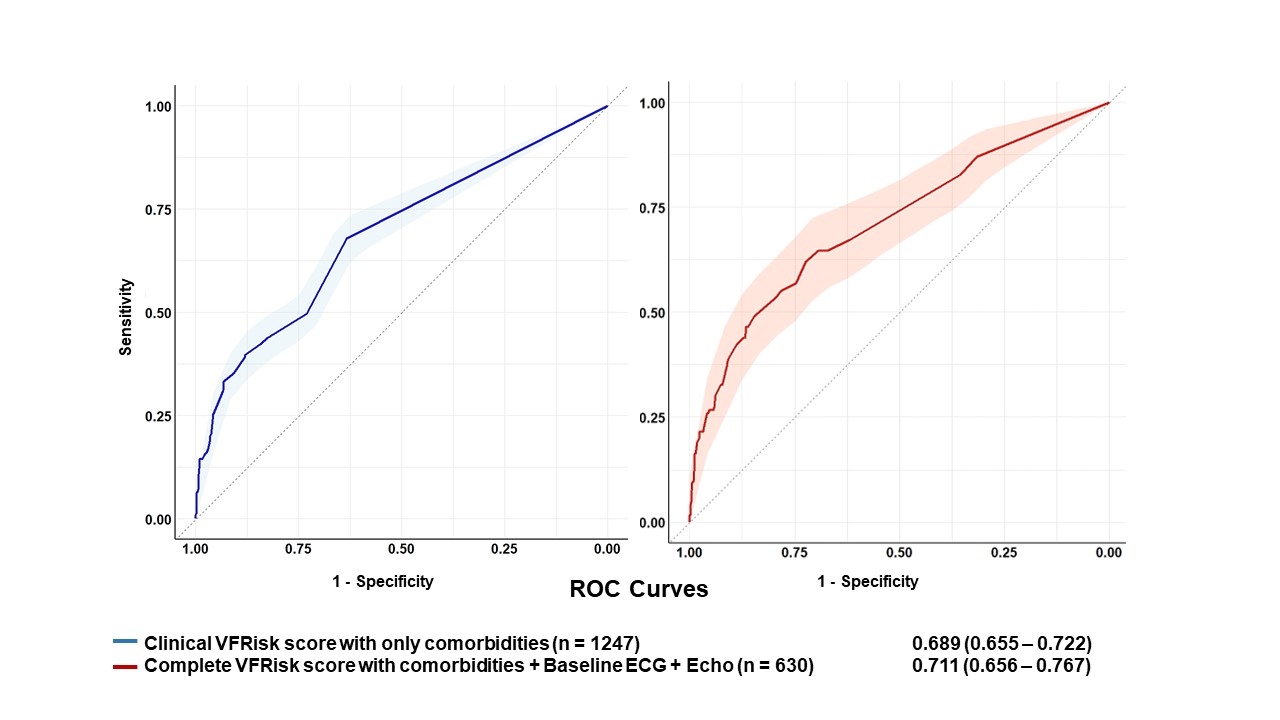
Abstract Body (Do not enter title and authors here): Introduction Individuals with shockable sudden cardiac arrest (SCA) have higher survival if treated with an implantable cardioverter defibrillator or automated external defibrillator. We previously developed VFRisk Score from an ongoing US West Coast study, which performs significantly better than left ventricular ejection fraction<35% (C-statistic 0.81 vs 0.64). Hypothesis The VFRisk score predicts sudden cardiac death (SCD) in a US East Coast community-based cohort, the Framingham Heart Study (FHS). Methods We performed a nested case-control study in the FHS to test VFRisk. Cases were subjects who suffered SCD among the Original and Offspring cohorts. Controls were randomly selected at a ratio of 1:3, matched on age, sex, cohort, and exam. Demographic features and comorbidities were assessed from the FHS exam closest to the SCD event. VFRisk was the sum of 13 risk factors, each multiplied by its respective coefficient including diabetes (1.4), myocardial infarction (MI, 1.4), atrial fibrillation (AF, 1.8), stroke (1.7), heart failure (HF, 2.1), chronic pulmonary disease (1.5), seizure disorder (3.5), syncope (2.8), heart rate ≥75 (1.5), prolonged QTc (1.7), Tpeak-end ≥90ms (1.7), delayed intrinsicoid deflection ≥50ms (2.1), and echocardiogram left ventricular hypertrophy (2.4). Intrinsicoid deflection was excluded due to data unavailability. Results Among 312 cases and 935, mean ages were 69.5 and 69.7 years, respectively, with 70.8% male in both groups. SCD cases had a significantly higher prevalence of diabetes, HF, stroke, AF, and MI compared to the control group. The VFRisk score was replicated with good discrimination (C-statistic 0.71, 95% CI 0.66-0.77) for SCD. SCD cases had higher VFRisk scores than controls (3.8±2.8 vs. 1.8±1.7, p<0.001). A 1-unit increase in VFRisk score was associated with a 48% increase of SCD (odds ratio 1.48; 95% CI 1.34-1.64). The highest risk score quartile was associated with 6-fold higher odds of SCD than the lowest quartile. Conclusion The VFRisk score to predict shockable SCA was successfully replicated in the FHS. The differences in discrimination between the two studies could be explained by the inability to distinguish shockable versus non-shockable SCA in the FHS.
Truyen, Thien Tan Tri Tai
(
Cedars-Sinai Medical Center
, Los Angeles , California , United States )
Lin, Honghuang
(
UMass Chan Medical school
, Worcester , Massachusetts , United States )
Mathias, Marco
(
Cedars-Sinai Medical Center
, Los Angeles , California , United States )
Chugh, Harpriya
(
Cedars-Sinai Medical Center
, Los Angeles , California , United States )
Reinier, Kyndaron
(
Cedars-Sinai Medical Center
, Los Angeles , California , United States )
Benjamin, Emelia
(
Boston University School Medicine
, Brookline , Massachusetts , United States )
Chugh, Sumeet
(
Cedars-Sinai Medical Center
, Los Angeles , California , United States )
Author Disclosures:
Thien Tan Tri Tai Truyen:DO NOT have relevant financial relationships
| Honghuang Lin:DO NOT have relevant financial relationships
| Marco Mathias:DO NOT have relevant financial relationships
| Harpriya Chugh:DO NOT have relevant financial relationships
| Kyndaron Reinier:DO NOT have relevant financial relationships
| Emelia Benjamin:DO NOT have relevant financial relationships
| Sumeet Chugh:DO NOT have relevant financial relationships