Impact of Stress Hyperglycemia Ratio on Heart Failure and Atherosclerotic Cardiovascular Events After Acute Myocardial Infarction
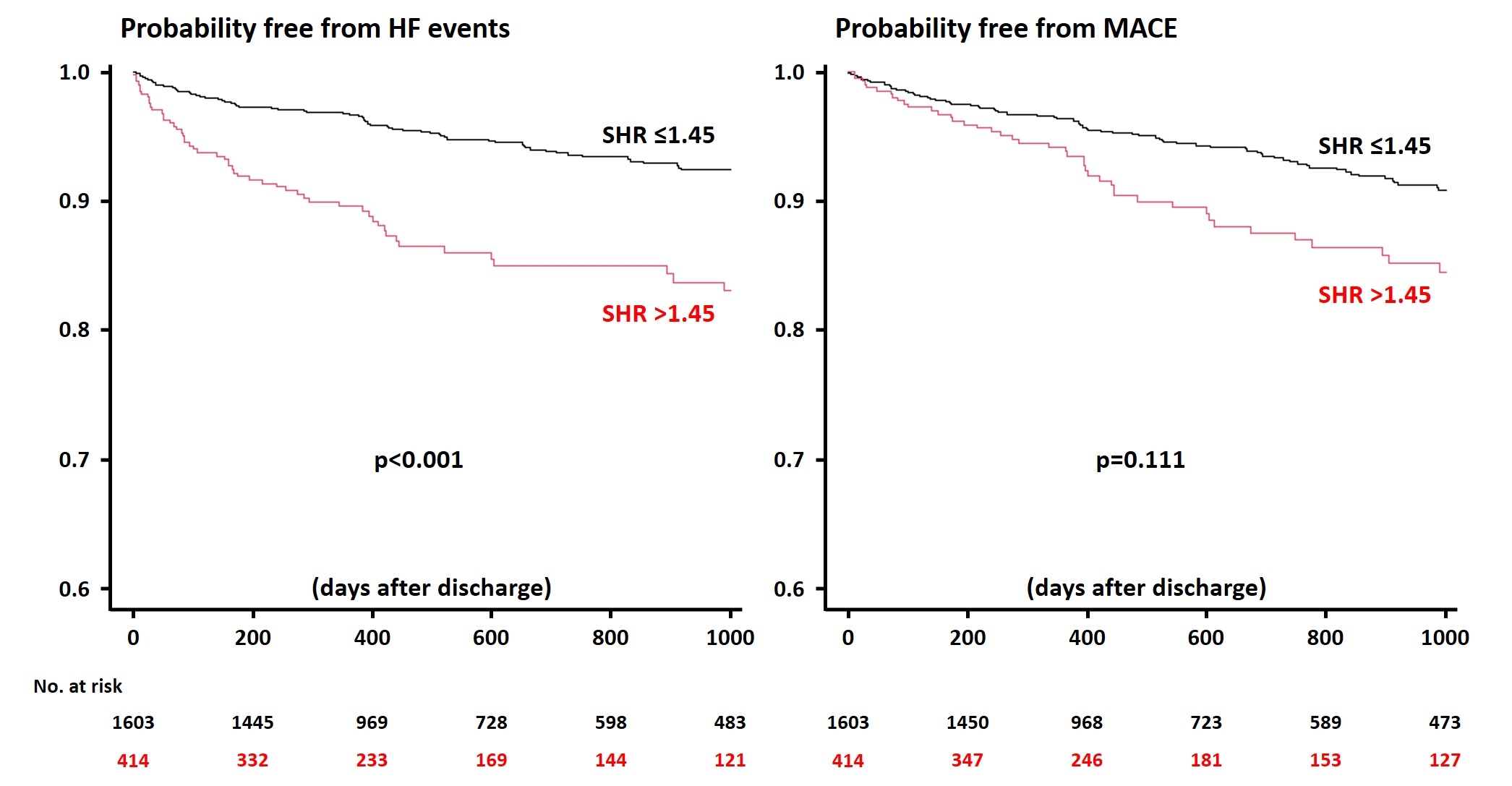
Abstract Body (Do not enter title and authors here): Background: An acute hyperglycemic status is reportedly associated with poor prognosis in patients with acute cardiovascular diseases. Although the stress hyperglycemia ratio (SHR) is a novel index to accurately represent the hyperglycemic condition on admission, relations between SHR and clinical outcomes are not fully evaluated in a setting of acute myocardial infarction (MI). Methods: This retrospective, multicenter registry study included 2,386 patients with acute MI undergoing percutaneous coronary intervention. SHR was calculated as a blood glucose level on admission divided by the estimated average glucose derived from a glycated hemoglobin level. The co-primary endpoints of this study included heart failure (HF)-related events (a composite of all-cause death and worsening and hospitalized HF) and major atherosclerotic cardiovascular events (MACE) (a composite of all-cause death, recurrent MI, and ischemic stroke), during the index hospitalization and after discharge. Results: Of the 2,386 patients, 890 (37.3%) had diabetes, and the median SHR was 1.17 [0.99, 1.45]. HF events and MACE occurred in 680 (28.5%) and 233 (9.8%) during hospitalization. SHR was identified as a factor significantly associated with both in-hospital HF events (adjusted odds ratio 1.65, 95% confidence interval 1.18-2.29, p=0.003) and MACE (adjusted odds ratio 1.50, 95% confidence interval 1.10-2.03, p=0.009). Among 2,017 patients who survived to discharge and had follow-up information, 195 (9.7%) and 214 (10.6%) experienced HF events and MACE during the median of 536 days after discharge. Patients with the high SHR (>1.45, 4th quartile) had an increased risk of HF events than those with SHR ≤1.45, while the incidence of MACE after discharge did not differ significantly between the two groups (Figure). The multivariable analysis confirmed the association of SHR with long-term HF events. Conclusions: In patients with acute MI, SHR was predictive of in-hospital outcomes including HF events and MACE, while after discharge, the higher SHR was associated with a higher HF risk but not with MACE. Further studies are needed to elucidate the underlying mechanisms and potential incremental benefit of SHR in stratifying patient risks after MI.
Okita, Shogo
(
Chiba University Graduate School of Medicine
, Chiba , Japan )
Saito, Yuichi
(
Chiba University Graduate School of Medicine
, Chiba , Japan )
Kitahara, Hideki
(
Chiba University Graduate School of Medicine
, Chiba , Japan )
Kobayashi, Yoshio
(
Chiba University Graduate School of Medicine
, Chiba , Japan )
Author Disclosures:
Shogo Okita:DO NOT have relevant financial relationships
| Yuichi Saito:DO NOT have relevant financial relationships
| Hideki Kitahara:DO NOT have relevant financial relationships
| Yoshio Kobayashi:DO NOT have relevant financial relationships