Ectasias of Multiple Coronary Arteries and a Coronary Cameral Fistula Between Right Coronary Artery and Coronary Sinus
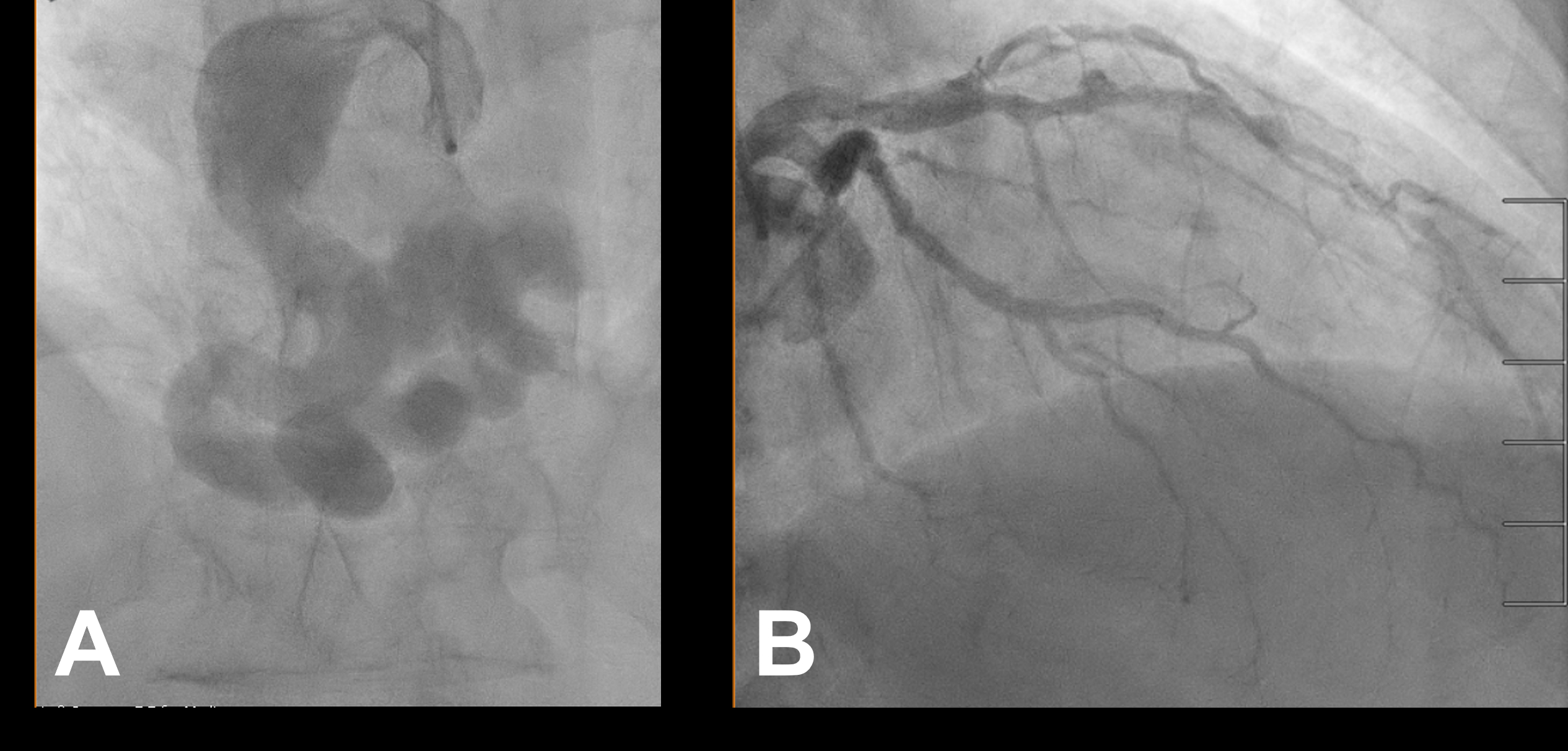
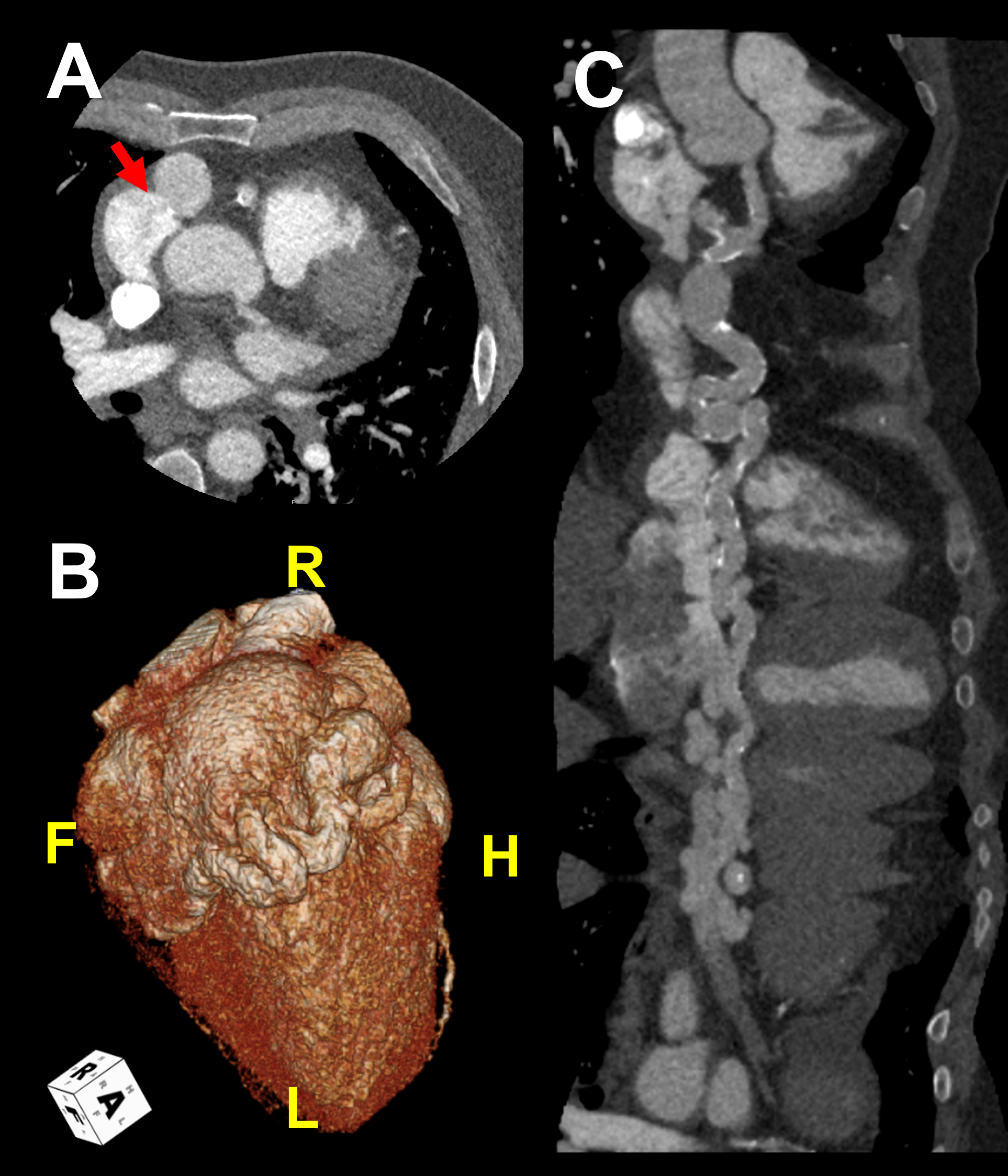
Abstract Body (Do not enter title and authors here): Case Description A 59-year-old male with history of hypertension, diabetes, Hashimoto’s thyroiditis presented with new, progressive shortness of breath. No murmur or extra heart sound were heard, and the lung sounds were normal. Exam was notable for significant lower extremity edema. Echocardiography showed reduced LVEF of 30%, and cardiac catheterization found hemodynamically significant shunt with Qp:Qs of 1.47:1. Coronary angiography revealed a tortuous and extremely aneurysmal RCA, as well as multivessel coronary artery disease (mvCAD) involving LAD, D1, LCx, OM1. Notably, the LAD had multiple aneurysmal segments and areas of eccentric stenosis upto 90%. Multislice CT angiography further characterized the RCA, which extends to the coronary sinus (CS) distally forming a coronary cameral fistula (CCF). Cardiac MRI did not show significant ischemic findings. The patient received medical therapy consisting of antiplatelet agents, high dose statin, beta blocker and ACE inhibitor, as well as diuretics. Patient underwent surgical closure of fistula and a 2-vessel coronary artery bypass graft surgery, with a LIMA pedicle graft to the LAD, and SV graft to the LCx. Postoperatively, patient was continued on medical therapy with improvement of symptoms. At the time of discharge, LV systolic function improved to 39% and there were no findings concerning for coronary artery thrombosis or fistula repair failure. Patient was planned to gradually start cardiac rehab.
Discussion CCF is a rare anomalous connection between coronary arteries and a cardiac chamber or other major blood vessels of the heart. CCF can be congenital or acquired and has many variations. It is often clinically silent. However some patients can develop heart failure, angina, and arrhythmia due to significant intracardiac shunt or coronary steal phenomenon. In this case presentation, it is likely that his heart failure was caused by the significant left to right shunt due to the fistula. He had concomitant ischemic cardiomyopathy in the setting of severe mvCAD, however the notable ectasia of LAD suggests there is a underlying disease that also affected RCA, leading to formation of the CCF. In addition to diagnostic coronary angiogram, advances in noninvasive cardiac imaging allow further identification and characterization of these fistulae. Surgical approach was appropriate in this patient given the findings complex mvCAD and the CCF with significant hemodynamic shunt.
Sung, Shijun
(
California Pacific Medical Center
, Brisbane , California , United States )
Gray, Hannah
(
California Pacific Medical Center
, San Francisco , California , United States )
Author Disclosures:
Shijun Sung:DO NOT have relevant financial relationships
| Hannah Gray:No Answer