Clinical Outcomes Of P2Y12 Inhibitor Monotherapy Versus Dual Antiplatelet Therapy After Percutaneous Coronary Intervention In Patients With Acute Coronary Syndrome: A Meta-Analysis Of Randomized Controlled Trials
Abstract Body (Do not enter title and authors here): Introduction: Dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor is recommended after percutaneous coronary intervention (PCI) to lower the risk of cardiovascular events. However, prolonged DAPT has been shown to increase bleeding risk, while some studies have shown that shorter-duration of DAPT followed by aspirin alone increases ischemic risk.
Research question: This study aimed to compare the risks and benefits of monotherapy with P2Y12 inhibitors and DAPT after PCI.
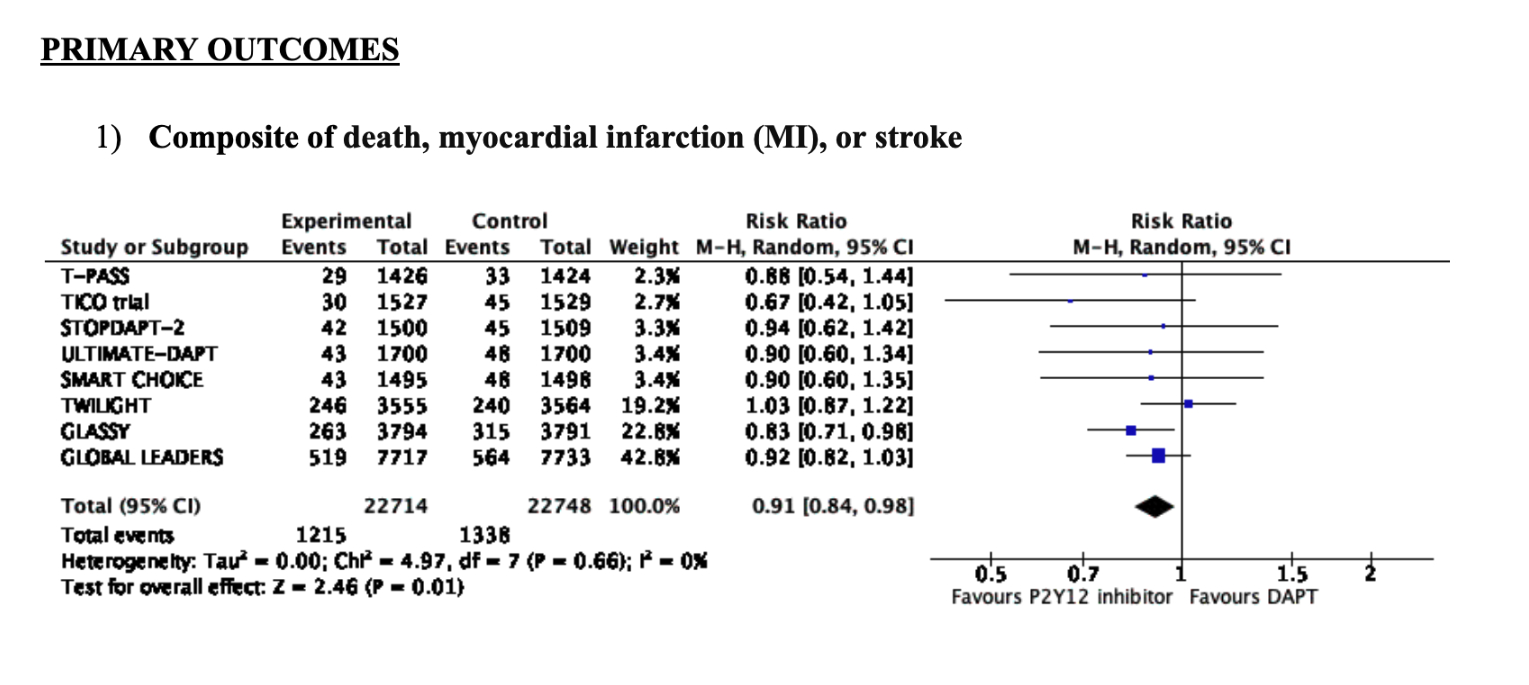
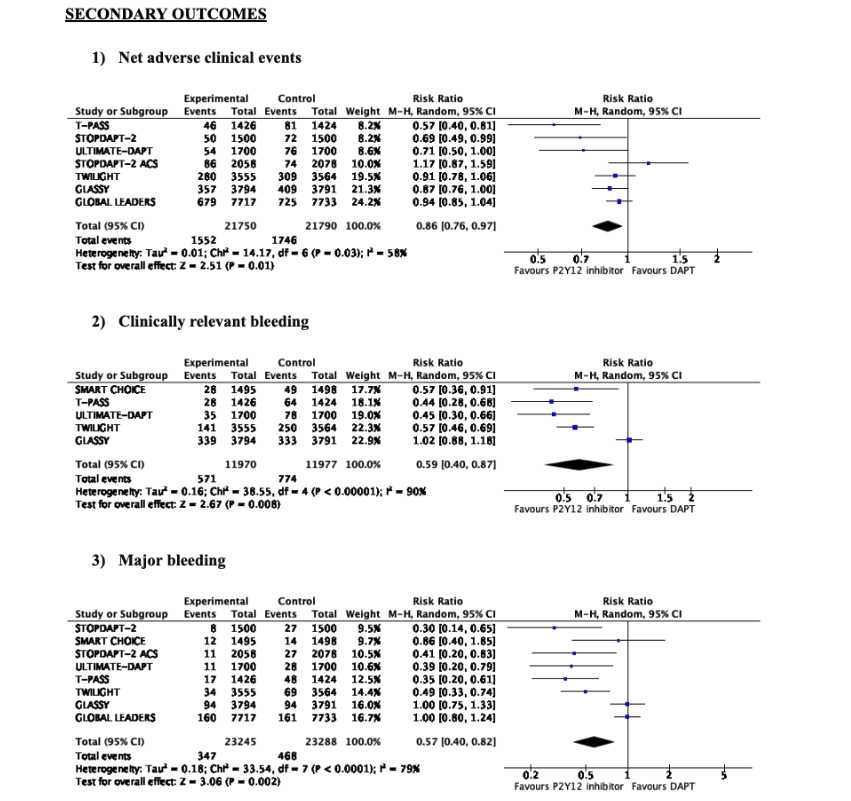
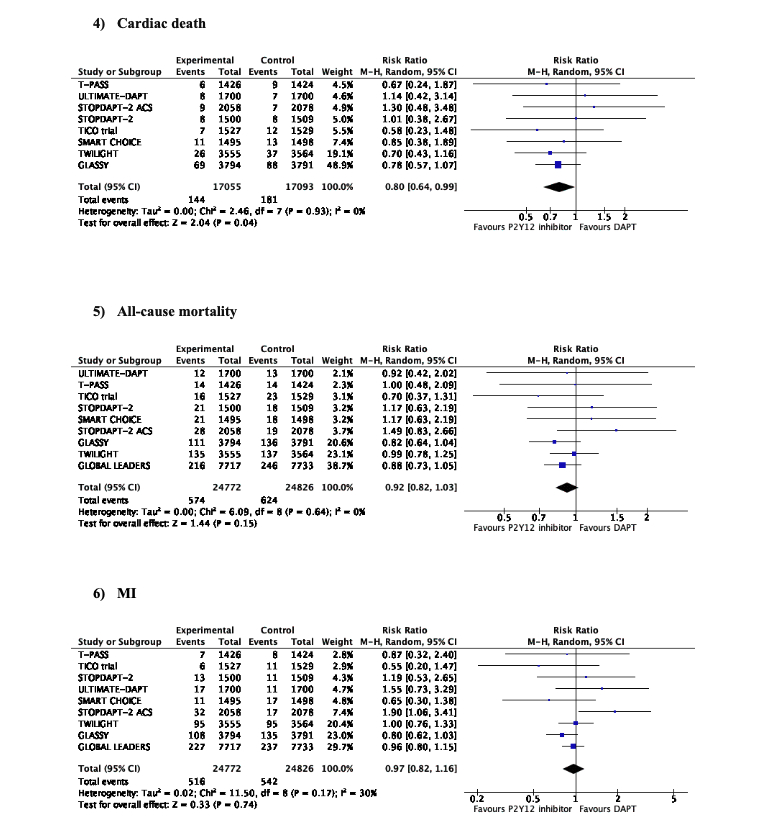
Methods: We searched the Medline, Embase, and Cochrane databases for randomized controlled trials (RCTs) involving adult patients hospitalized with ACS who underwent PCI. Our primary outcome was the composite of death, myocardial infarction (MI), and stroke. The secondary outcomes were net adverse clinical events (NACEs which is the primary outcome and risk of major bleeding), all-cause mortality, cardiac death, MI, stroke, stent thrombosis, target vessel revascularization, clinically relevant bleeding, and major bleeding. We used Review Manager 5.4 for the statistical analysis, employing risk ratios (RRs) with 95% confidence intervals (CIs).
Results: Nine RCTs were included, involving a total of 34,322 patients, with 48.9% receiving P2Y12 inhibitor monotherapy after 1–3 months of DAPT. Regarding the primary outcomes, the risk of the composite of all-cause mortality, MI and stroke was significantly lower in patients receiving P2Y12 monotherapy as compared to patients on DAPT (RR 0.91[95% CI 0.84–0.98], I2=0%, p=0.01). With respect to the secondary outcomes, there was a significantly lower risk of NACEs (RR 0.86 [95% CI 0.76–0.97], I2=58%, p=0.01), clinically relevant bleeding (RR 0.59 [95% CI 0.38–0.93], I2=92%, p<0.00001), major bleeding (RR 0.57 [95% CI 0.40–0.82], I2=79%, p=0.002) as well as cardiac death (RR 0.80 [95% CI 0.64–0.99], I2=0%, p=0.04) in patients receiving P2Y12 inhibitor monotherapy. There was no significant difference in the risk of all-cause mortality, MI, stroke, target vessel revascularization, and stent thrombosis between the 2 groups.
Conclusion: This meta-analysis found a significant decrease in the risk of the composite of death, MI, and stroke in patients receiving P2Y12 inhibitor monotherapy. It also showed that the risk of net adverse clinical events and major bleeding is lower in patients receiving P2Y12 inhibitor monotherapy.
Gupta, Soumya
(
Mount Sinai Morningside- West
, New York , New York , United States )
Thakkar, Aditya
(
East Tennessee State University
, Johnson City , Tennessee , United States )
Aggarwal, Devika
(
Mount Sinai Morningside
, New York , New York , United States )
Bhatia, Kirtipal
(
Mount Sinai Morningside
, New York , New York , United States )
Choi, James
(
Mount Sinai Morningside- West
, New York , New York , United States )
Carter, Kristen
(
Mount Sinai Morningside- West
, New York , New York , United States )
Kaur, Arpanjeet
(
Mount Sinai Morningside- West
, New York , New York , United States )
Casso, Abel
(
Mount Sinai Morningside
, New York , New York , United States )
Author Disclosures:
Soumya Gupta:DO NOT have relevant financial relationships
| Aditya Thakkar:DO NOT have relevant financial relationships
| Devika Aggarwal:No Answer
| Kirtipal Bhatia:DO NOT have relevant financial relationships
| James Choi:DO NOT have relevant financial relationships
| Kristen Carter:DO NOT have relevant financial relationships
| Arpanjeet kaur:No Answer
| Abel Casso:DO NOT have relevant financial relationships