The Use of Angiotensin Receptor Blockers Decreased Three-Year and Five-Year Mortality in a VA Population with Ascending Thoracic Aortic Aneurysms
Abstract Body (Do not enter title and authors here): Background: The incidence of ascending thoracic aortic aneurysms (aTAA) is approximately 5-10/100000 individuals/year. Estimates of acute rupture or dissection range from 1.6-4/100000 individuals/year with a mortality rate for untreated dissection up to 50% within 48 hours. Current guidelines recommend surgical intervention for aTAAs ≥ 55mm in diameter. Risk factors that contribute to aTAA growth and mortality include diabetes, age, and smoking history however, not much investigation has been done to evaluate protective factors.
Objective: To evaluate clinical factors that reduce three-year and five-year all-cause mortality in a veteran population who have dilated ascending aortas or ascending thoracic aortic aneurysms (aTAA) and who did not undergo repair within three or five years.
Methods: We conducted a cohort study of 887 patients followed for aTAA (diameter ≥ 4.0cm) at a Veterans Affairs hospital. Patients who died of any cause before repair within 3 or 5 years of aTAA identification or had 3 or 5 years of follow-up without repair were further analyzed. 57 pertinent factors (including social, genetic, cardiac risk factors, aneurysm size, medications, etc.) were evaluated in univariate logistic regression models of three and five-year all-cause mortality. Variables with univariate p<0.2 were combined in a multivariate logistic regression model. P<0.05 was considered statistically significant.
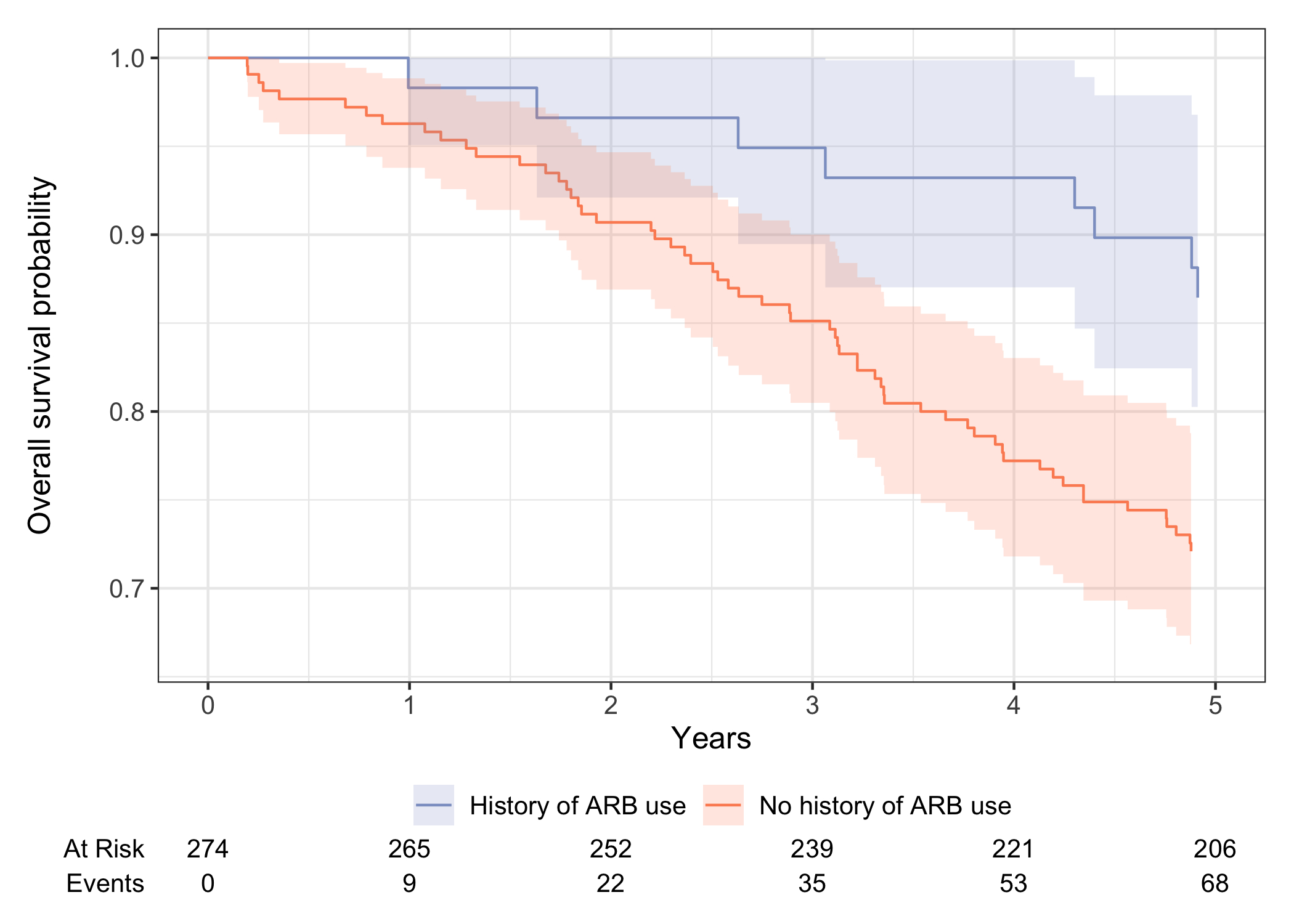
Results: In the 3-year model, 392 had ≥3 years follow-up without aTAA surgical repair. 35 out of 392 patients (8.9%) died within 3 years. The only statistically significant variable that reduced mortality was history of angiotensin receptor blocker (ARB) use (OR 0.24, p=0.042). In the 5-year model, 274 had ≥5 years follow-up without aTAA surgical repair. 68 out of 274 patients (24.8%) died within 5 years. Similarly, history of ARB use (OR 0.22, p=0.003) was the only pertinent variable. For both models, the results were independent of age, history of diabetes, valve disease, CHF, and stroke.
Conclusion: Among modifiable risk factors, at both 3 and 5 years, history of ARB was associated with reduced mortality (13% mortality compared to 27% at 5 years) and should be further investigated.
Kailash, Vidur
(
UCSF AND SFVAMC
, San Francisco , California , United States )
Tu, Sally
(
UCSF AND SFVAMC
, San Francisco , California , United States )
Zamirpour, Siavash
(
UCSF AND SFVAMC
, San Francisco , California , United States )
Pace, William
(
UCSF AND SFVAMC
, San Francisco , California , United States )
Boskovski, Marko
(
UCSF AND SFVAMC
, San Francisco , California , United States )
Ge, Liang
(
UCSF AND SFVAMC
, San Francisco , California , United States )
Tseng, Elaine
(
UCSF AND SFVAMC
, San Francisco , California , United States )
Author Disclosures:
Vidur Kailash:DO NOT have relevant financial relationships
| Sally Tu:DO NOT have relevant financial relationships
| Siavash Zamirpour:DO NOT have relevant financial relationships
| William Pace:DO NOT have relevant financial relationships
| Marko Boskovski:DO have relevant financial relationships
;
Consultant:Edwards Lifesciences:Active (exists now)
| Liang Ge:DO have relevant financial relationships
;
Ownership Interest:ReValve Med Inc.:Active (exists now)
| Elaine Tseng:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Artivion Inc:Past (completed)
; Research Funding (PI or named investigator):Ottawa Heart Institute:Active (exists now)
; Research Funding (PI or named investigator):Potrero:Past (completed)
; Research Funding (PI or named investigator):Cellphire:Past (completed)
; Research Funding (PI or named investigator):Amgen Inc:Active (exists now)