Social Determinants of Health and Disparities in Guideline-Directed Medical Therapy Optimization for Heart Failure
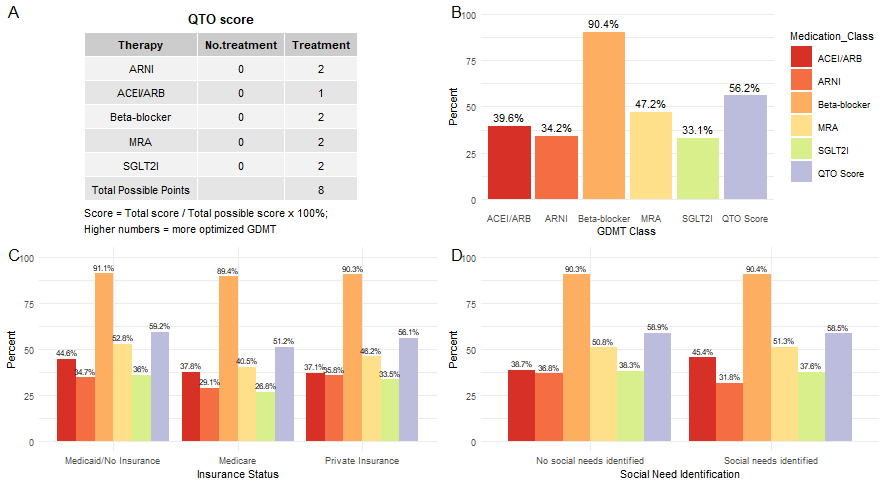
Abstract Body (Do not enter title and authors here): Introduction: Less than 20% of eligible patients with heart failure with reduced ejection fraction (HFrEF) receive all four pillars of guideline-directed medical therapy (GDMT). Understanding disparities in sex, race, ethnicity, and adverse social determinants of health (SDoH) is necessary to equitably optimize quadruple therapy. Methods: Utilizing the American Heart Association Get With The Guidelines® Heart Failure registry, we conducted a retrospective cross-sectional study to examine the associations between exposures of race and ethnicity, sex, and adverse SDoH (insurance status and a documented social need [any barrier to accessing healthcare]) with quadruple therapy optimization (QTO) at discharge in patients with HFrEF hospitalized between 7/1/2021-9/30/2023. The outcome was a novel QTO score incorporating SGLT2Is as a pillar of quadruple therapy (Figure 1A). Associations between each exposure and QTO score were assessed using multivariable adjusted linear models to calculate adjusted mean differences (AMDs) and 95% confidence intervals (CIs). Results: Among 82,637 included patients (median age 66.0 years, 32.5% female, 57.0% non-Hispanic White, 76.4% prior HF), the overall mean QTO score was 56.2% (standard deviation 25.5). The use of each GDMT component is shown in Figure 1B. After adjustment, Non-Hispanic Black (AMD 2.56 percentage points [95% CI, 2.17, 2.96]) and Hispanic individuals (AMD 0.73 percentage points [95% CI, 0.13, 1.33]) had higher QTO scores vs. Non-Hispanic White individuals. Females had higher QTO scores than males (AMD 1.93 percentage points [95% CI, 1.56, 2.29]). Patients with Medicaid/no insurance (AMD -1.30 percentage points [95% CI, -1.71, -0.88]) and Medicare (AMD -1.70 percentage points [95% CI, -2.16, -1.23]) had lower QTO scores vs. private insurance (Figure 1C). Those with vs. without an identified social need had lower QTO scores (AMD -3.40 percentage points [95% CI, -4.10, -2.71]) (Figure 1D). Conclusion: Disparities in quadruple therapy optimization were most evident for patients with adverse SDoH. Patients with Medicaid/no insurance, Medicare, or an identified social need had lower QTO scores. Future efforts should focus on reducing these gaps to improve equitable GDMT use.
Jacobs, Joshua
(
University of Utah
, Salt Lake City , Utah , United States )
Ayodele, Iyanuoluwa
(
Duke University School of Medicine
, Durham , North Carolina , United States )
Bress, Adam
(
University of Utah
, Salt Lake City , Utah , United States )
Sterling, Madeline
(
Weill Cornell Medical College
, New York , New York , United States )
Pandey, Ambarish
(
UTSW MEDICAL CENTER
, Dallas , Texas , United States )
Derington, Catherine
(
University of Utah
, Salt Lake City , Utah , United States )
Zheutlin, Alexander
(
Northwestern University
, Chicago , Illinois , United States )
Shah, Kevin
(
University of Utah
, Salt Lake City , Utah , United States )
Greene, Stephen
(
Duke University School of Medicine
, Durham , North Carolina , United States )
Alhanti, Brooke
(
Duke University School of Medicine
, Durham , North Carolina , United States )
Blanco, Rosalia
(
Duke University School of Medicine
, Durham , North Carolina , United States )
Fonarow, Gregg
(
UCLA MEDICAL CENTER
, Los Angeles , California , United States )
Author Disclosures:
Joshua Jacobs:DO have relevant financial relationships
;
Researcher:AHA Get With The Guidelines Early Career Seed Grant:Active (exists now)
| Brooke Alhanti:DO NOT have relevant financial relationships
| Rosalia Blanco:DO NOT have relevant financial relationships
| Gregg Fonarow:DO have relevant financial relationships
;
Consultant:Abbott:Past (completed)
; Consultant:Johnson and Johnson:Past (completed)
; Consultant:Pfizer:Active (exists now)
; Consultant:Novartis:Active (exists now)
; Consultant:Medtronic:Active (exists now)
; Consultant:Merck:Active (exists now)
; Consultant:Eli Lilly:Past (completed)
; Consultant:Boehringer Ingelheim:Past (completed)
; Consultant:Cytokinetics:Active (exists now)
; Consultant:Bayer:Active (exists now)
; Consultant:Astra Zeneca:Past (completed)
; Consultant:Amgen:Past (completed)
| Iyanuoluwa Ayodele:DO NOT have relevant financial relationships
| Adam Bress:DO NOT have relevant financial relationships
| Madeline Sterling:DO NOT have relevant financial relationships
| Ambarish Pandey:DO have relevant financial relationships
;
Consultant:Tricog:Active (exists now)
; Consultant:Lilly:Active (exists now)
; Consultant:Edwards Lifesciences:Active (exists now)
; Consultant:Semler:Active (exists now)
; Consultant:Science37:Active (exists now)
; Research Funding (PI or named investigator):SCPharma:Active (exists now)
; Advisor:Medtronic:Active (exists now)
; Advisor:Axon:Active (exists now)
; Advisor:Bayer:Active (exists now)
; Research Funding (PI or named investigator):Ultromics:Active (exists now)
; Consultant:Novo Nordisk:Active (exists now)
; Consultant:Roche:Active (exists now)
| Catherine Derington:DO NOT have relevant financial relationships
| Alexander Zheutlin:DO NOT have relevant financial relationships
| Kevin Shah:No Answer
| Stephen Greene:DO have relevant financial relationships
;
Consultant:AstraZeneca:Active (exists now)
; Consultant:Corcept:Past (completed)
; Consultant:Otsuka:Active (exists now)
; Consultant:Lilly:Active (exists now)
; Consultant:Novo Nordisk:Active (exists now)
; Consultant:Merck:Active (exists now)
; Consultant:Roche Diagnostics:Active (exists now)
; Consultant:Lexicon:Active (exists now)
; Consultant:Boehringer Ingelheim:Active (exists now)
; Consultant:Cytokinetics:Past (completed)
; Consultant:Bayer:Active (exists now)