Publicly-Insured Patients Have Lower Rates of Cardiac Rehabilitation Enrollment: A Statewide Experience in Michigan
__PRESENT
Abstract Body (Do not enter title and authors here): Introduction: Cardiac rehabilitation (CR) is a clinically effective and underused service for patients with recent cardiac events, and insurance coverage is an important, yet understudied, mediator. The objective of this study was to evaluate the relationship between insurance type and CR participation.
Methods: Data from the Michigan Value Collaborative multi-payer claims based registry were used to identify Michigan residents admitted for percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) between 01/01/2018-12/31/2022. Payer categories included commercial insurance, Medicare Advantage (MA), Medicare fee-for-service (FFS), and Medicaid. CR participation was defined as having at least one approved CR claim within 365 days of discharge. Unadjusted comparisons of CR enrollment across payers were done using chi-square tests. Multivariable logistic regression adjusted for patient demographics and comorbidities evaluated the association between payer category and CR participation.
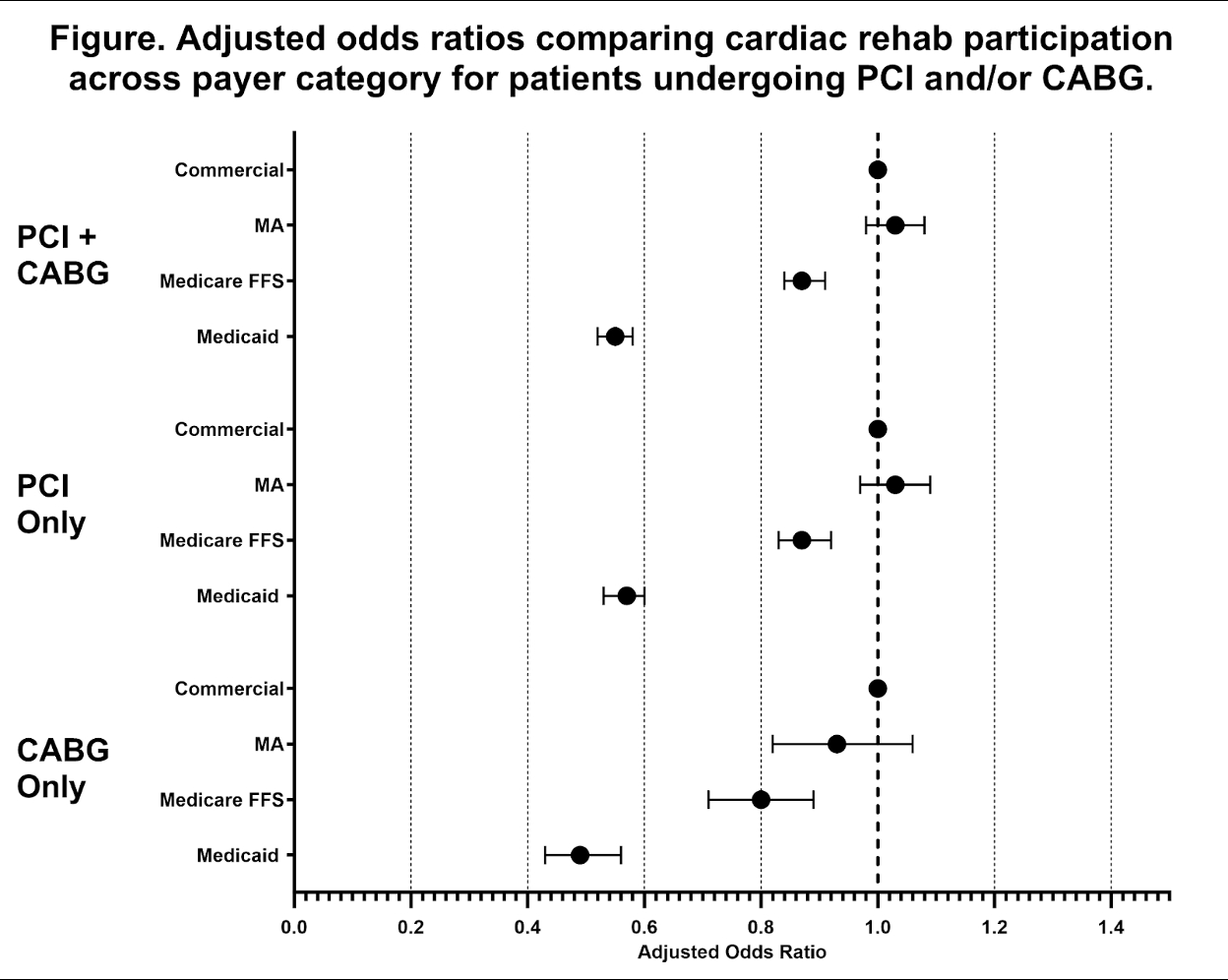
Results: The final sample included 74,505 episodes of PCI (82%) or CABG (18%) with mean (SD) patient age 67.7 (11.4) yrs, 68% male, and a payer breakdown of 23% commercial insurance, 22% MA, 41% Medicare FFS, and 14% Medicaid. Overall, 29,829 (40%) patients participated in a single session of CR, with a higher participation in CABG vs. PCI (60% vs. 36%, p<0.001). There were significant differences in CR use across payers, with commercially insured individuals having highest rates (46%) followed by MA (43%), Medicare FFS (39%), and lowest for Medicaid (30%, p<0.001). Compared with commercially insured patients, individuals with Medicaid (adjusted odds ratio, aOR=0.55 [0.52-0.58], p<0.001) and Medicare FFS (aOR=0.87 [0.84-0.91], p<0.001) were significantly less likely to participate in CR (Figure). The relationship persisted when stratified by the method of revascularization.
Conclusion: Individuals with Medicaid and Medicare FFS coverage had lower rates of CR participation than those with MA or commercial insurance following PCI or CABG. Understanding disparities in CR usage by payer may help target quality improvement efforts and increase equitable use of secondary disease prevention strategies.__PRESENT
Pedamallu, Havisha
(
Northwestern University
, Chicago , Illinois , United States )
Mantey, Julia
(
University of Michigan
, Ann Arbor , Minnesota , United States )
Sukul, Devraj
(
University of Michigan Health Syste
, Ann Arbor , Michigan , United States )
Keteyian, Steven
(
HENRY FORD HOSPITAL
, Detroit , Michigan , United States )
Pagani, Francis
(
University of Michigan
, Ann Arbor , Minnesota , United States )
Hawkins, Robert
(
University of Michigan
, Ann Arbor , Minnesota , United States )
Likosky, Donald
(
University of Michigan
, Ann Arbor , Minnesota , United States )
Thompson, Mike
(
University of Michigan
, Ann Arbor , Michigan , United States )
Author Disclosures:
Havisha Pedamallu:DO NOT have relevant financial relationships
| Julia Mantey:DO NOT have relevant financial relationships
| Devraj Sukul:No Answer
| Steven Keteyian:DO NOT have relevant financial relationships
| Francis Pagani:DO NOT have relevant financial relationships
| Robert Hawkins:DO have relevant financial relationships
;
Consultant:Medtronic:Active (exists now)
| Donald Likosky:No Answer
| Mike Thompson:DO NOT have relevant financial relationships