Trends and Disparities in Mortality Due to Thoracic Aortic Aneurysm in Patients in the United States from 1999 to 2020
Abstract Body (Do not enter title and authors here): Background Thoracic aortic aneurysms (TAA) impact approximately 6 to 10 individuals per 100,000 people, though the actual prevalence is likely higher due to frequent asymptomatic presentations, posing a challenge for early diagnosis. The rupture of these aneurysms presents a significant risk, resulting in an estimated 30,000 deaths annually in the United States alone. This emphasizes the urgent need for enhanced detection and treatment strategies. An understanding of trends in TAA mortality is imperative for assessing the efficacy of current approaches, pinpointing vulnerable populations, and ultimately, advancing treatment equity.
Methods This study utilized death certificates from 1999 to 2020 sourced from the CDC WONDER Database. Deaths among individuals aged 25 years and older attributed to TAA were identified using the International Classification of Diseases, Tenth Revision (ICD-10) codes I71.1 and I71.2. Age-adjusted mortality rates (AAMRs) per 1,000,000 individuals and annual percent change (APC) were computed and stratified based on year, gender, race/ethnicity, and urbanization status.
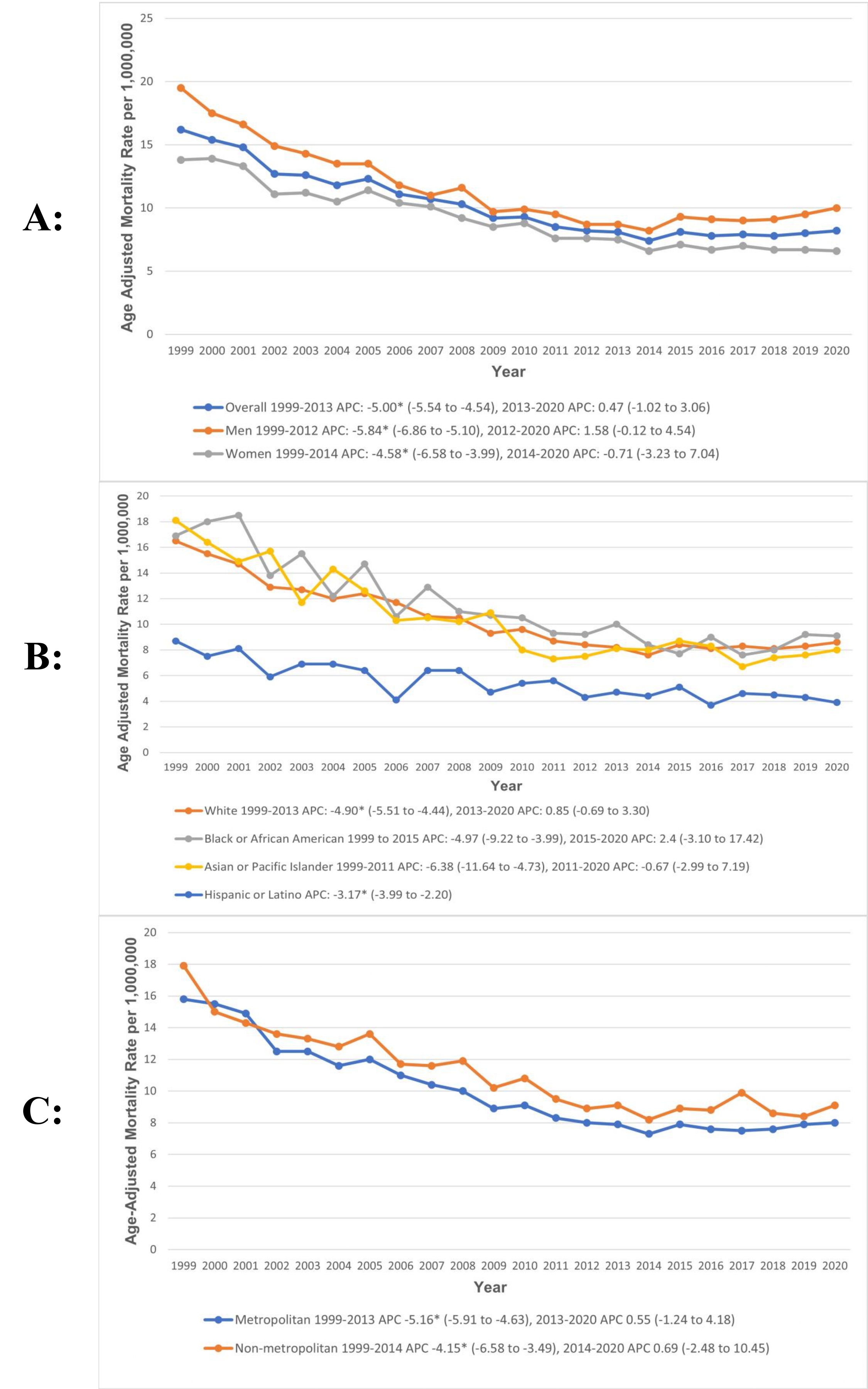
Results Between 1999 and 2020, 47,136 deaths were reported in patients with TAA. Overall, AAMR decreased from 16.2 to 8.2 per 1,000,000 population between 1999 and 2020, with a significant decline from 1999 to 2013 (APC: -5.00; 95% CI: -5.54 to -4.5), followed by a slight increase from 2013 to 2020 (APC: 0.47; 95% CI: -1.02 to 3.06). Gender-based analysis revealed that men had consistently higher AAMRs than women (men: 11.2; 95% CI: 11 to 11.3; vs. women: 9; 95% CI: 8.9 to 9.1). Moreover, we found that AAMRs were the highest among non-Hispanic African Americans (11; 95% CI: 10.7 to 11.3) followed by non-Hispanic Whites (10.3; 95% CI: 10.2 to 10.4), non-Hispanic Asian or Pacific Islanders (9.5; 95% CI: 9 to 9.9), non-Hispanic American Indian or Alaska Native (7.8; 95% CI: 6.6 to 9), and Hispanic populations (5.2; 95% CI 5 to 5.5). In addition, non-metropolitan areas had higher AAMRs than metropolitan areas (non-metropolitan areas: 11; 95% CI: 10.8 to 11.2; vs. metropolitan: 9.8; 95% CI: 9.7 to 9.9) (Figure 1).
Conclusions This analysis revealed a significant decline in mortality since 1999 from TAA, with a slight upward trend in recent years. However, disparities persist, with higher AAMRs observed among men, non-Hispanic African Americans, and residents of non-metropolitan areas.
Goyal, Aman
(
Seth GSMC and KEM Hospital
, Mumbai , India )
., Abdullah
(
Rawalpindi Medical University
, Rawalpindi , Pakistan )
Maheshwari, Surabhi
(
University of Alabama
, Montgomery , Alabama , United States )
Saeed, Humza
(
Rawalpindi Medical University
, Rawalpindi , Pakistan )
Jain, Hritvik
(
AIIMS Jodhpur
, Jodhpur , India )
Ullah, Irfan
(
KABIR MEDICAL COLLEGE
, Peshawar , Pakistan )
Abbasi, Haleema Qayyum
(
Ayub Medical College
, Abbottabad , Pakistan )
Changez, Mah I Kan
(
Yale University
, New Haven , Connecticut , United States )
Mahalwar, Gauranga
(
Cleveland Clinic Foundation
, Cleveland , Ohio , United States )
Author Disclosures:
Aman Goyal:DO NOT have relevant financial relationships
| Abdullah .:DO NOT have relevant financial relationships
| Surabhi Maheshwari:DO NOT have relevant financial relationships
| Humza Saeed:DO NOT have relevant financial relationships
| Hritvik Jain:DO NOT have relevant financial relationships
| Irfan Ullah:DO NOT have relevant financial relationships
| Haleema Qayyum Abbasi:DO NOT have relevant financial relationships
| Mah I Kan Changez:DO NOT have relevant financial relationships
| GAURANGA MAHALWAR:DO NOT have relevant financial relationships