Variation in Prevalence, Treatment, and Outcomes in Heart Failure with Improved Ejection Fraction by Race and Ethnicity
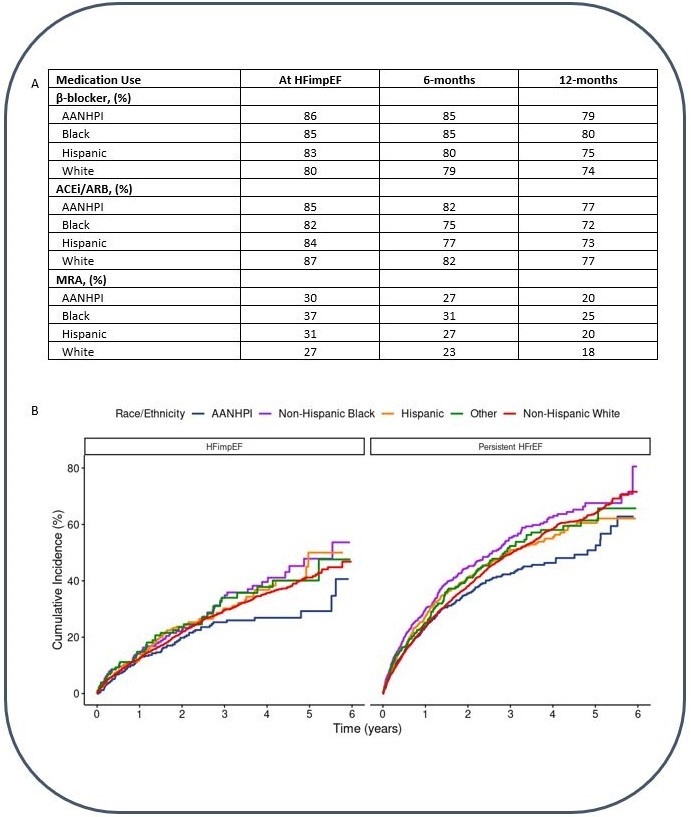
Abstract Body (Do not enter title and authors here): Background: Racial and ethnic disparities exist in heart failure with reduced ejection fraction (HFrEF), but little is known about how race and ethnicity relate to patients with HF with improved EF (HFimpEF). Research Question: Do the epidemiology, treatment, and outcomes vary by race and ethnicity in patients with HFimpEF? Aim: To describe the relationship between race and ethnicity and HFimpEF within a large, integrated health care delivery system. Methods: We identified adults aged ≥18 years with incident HFrEF (LVEF≤40%) from 2013-2018 within Kaiser Permanente Northern California. HFimpEF was defined as LVEF>40% within 12 months after incident HFrEF. Self-reported race and ethnicity were classified as non-Hispanic White, non-Hispanic Black, Asian American/Native Hawaiian/Pacific Islander (AANHPI), Hispanic, and other. Incidence rates of worsening HF (WHF) events (i.e., HF hospitalization, ED visit, or urgent outpatient WHF visits) or all-cause death were compared across patients with HFimpEF and persistent HFrEF using Cox proportional hazard models adjusted for age, sex, and LVEF at incident HFrEF, stratified by race and ethnicity. Results: Among 12,639 adults with incident HFrEF, 7,562 (59.8%) were White, 1,481 (11.7%) were AANHPI, 1,385 (11.0%) were Black, and 1,537 (12.2%) identified as Hispanic. Rates of HFimpEF following incident HFrEF was lowest among Black patients (26%), but similar among other race and ethnicities (36%, 34%, 30%, and 30% for AANHPI, White, Hispanic, and other, respectively, chi-squared p<0.01). Medication use was similar across groups at time of HFimpEF, but generally declined thereafter (Panel A). Among patients with HFimpEF, Black and Hispanic patients had significantly higher crude rates of WHF or death compared to White patients (34 and 30 compared to 23 per 100 person-years, p<0.01 for each). Despite these differences in absolute rates, relative associations between HFimpEF (vs. persistent HFrEF) and WHF or death remained similar across all race and ethnicities (AANHPI: aHR=0.52 [95%CI 0.42-0.65], Black: aHR=0.70 [95%CI 0.56-0.87], Hispanic: aHR=0.60 [95%CI 0.49-0.73], White: aHR=0.53 [95%CI 0.48-0.58], pinteraction=0.13) (Panel B). Conclusions: HFimpEF is common within 12 months after incident HFrEF, and HF medication adherence declines in the years following. HFimpEF is associated with improved clinical outcomes across race and ethnicity, but occurs less frequently in Black patients despite similar HF medical therapy use.
Chang, Alex
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Lee, Keane
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Parikh, Rishi
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Ambrosy, Andrew
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Tan, Thida
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Hamilton, Steven
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Pabon Porras, Maria
(
Brigham and Womens Hospital
, Brookline , Massachusetts , United States )
Vardeny, Orly
(
Minneapolis VA Health Care System
, Minneapolis , Minnesota , United States )
Ku, Ivy
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Vasti, Elena
(
Stanford University
, Stanford , California , United States )
Sandhu, Alexander
(
Stanford University
, Stanford , California , United States )
Go, Alan
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Adatya, Sirtaz
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Bhatt, Ankeet
(
KAISER PERMANENTE NORTHERN CAL
, Oakland , California , United States )
Author Disclosures:
Alex Chang:DO NOT have relevant financial relationships
| Elena Vasti:DO NOT have relevant financial relationships
| Alexander Sandhu:DO have relevant financial relationships
;
Consultant:Acumen LLC:Past (completed)
; Consultant:Lexicon Pharmaceuticals:Past (completed)
; Research Funding (PI or named investigator):Novartis Pharmaceuticals:Active (exists now)
; Research Funding (PI or named investigator):Reprieve Cardiovascular :Active (exists now)
| Alan Go:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Bristol Myers-Squibb:Active (exists now)
; Research Funding (PI or named investigator):Pfizer:Past (completed)
| Sirtaz Adatya:DO NOT have relevant financial relationships
| Ankeet Bhatt:DO have relevant financial relationships
;
Consultant:Novo Nordisk:Past (completed)
; Consultant:Merck:Past (completed)
| Keane Lee:No Answer
| Rishi Parikh:No Answer
| Andrew Ambrosy:DO have relevant financial relationships
;
Consultant:Merck:Active (exists now)
; Consultant:sc Pharma:Past (completed)
| Thida Tan:DO NOT have relevant financial relationships
| Steven Hamilton:DO NOT have relevant financial relationships
| Maria Pabon Porras:No Answer
| Orly Vardeny:DO have relevant financial relationships
;
Consultant:Cardior:Active (exists now)
; Other (please indicate in the box next to the company name):Bayer - research support to institution:Active (exists now)
; Advisor:Moderna:Active (exists now)
; Consultant:Bayer:Active (exists now)
; Research Funding (PI or named investigator):Cardurion - research support to institution:Active (exists now)
| Ivy Ku:DO NOT have relevant financial relationships