Predicting Long-Term Cardiac Morbidity and Mortality in Patients with Surgical Coronary Anatomy who are Deemed to be of High Surgical Risk
Abstract Body (Do not enter title and authors here): Background: Medically managed patients with surgical coronary artery disease (CAD) are a high-risk group. It is unclear whether existing mortality risk scores, anti-anginal usage or index presentation type can predict future morbidity and mortality in this cohort.
Methods: Consecutive medically managed patients with surgical CAD discussed at the cardiac conference of a tertiary Australian institution were included between 2012-2021. Surgical CAD was defined as stenosis >70% (or FFR <0.8) in a triple vessel distribution or double vessel with a dominant circumflex or >50% left main stenosis. Acute coronary syndrome (ACS) was defined as STEMI, NSTEMI or unstable angina (UA) at presentation. EuroSCORE and TIMI score were calculated with a score of >4% and ≥4 considered high respectively. Number of anti-anginal agents required to control symptoms was recorded. Readmission rates and long-term mortality data were collected until December 2023.
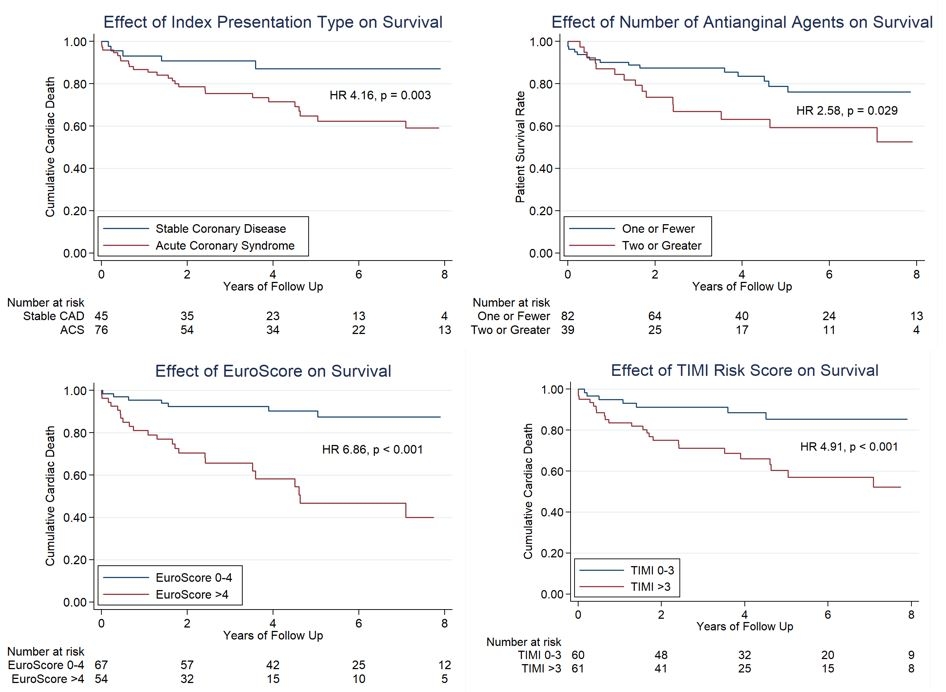
Results: In total, 121 patients were included after discussion and were followed up for a median of 3.6 years (IQR 1.9-6.4). Of these, 76 patients (62.8%) had an ACS presentation (13 STEMI (17.1%), 45 NSTEMI (59.2%), 18 UA (23.7%)), while 54 (44.6%) had high EuroSCORE and 61 (50.4%) had high TIMI-risk score. More than one antianginal agent was required for 39 patients (32.2%). ACS patients had an elevated risk of cardiac death at maximal follow up (HR 4.16 (95%CI 1.47-11.81), p=0.003)), as well as cardiac readmission within 30-days (OR 6.74 (1.48-30.61), p=0.003)) and 12 months (OR 2.57 (1.10-5.99), p=0.024). High EuroSCORE was a significant predictor of cardiac mortality (HR 6.86 (2.65-17.72), p<0.001)), however, did not predict cardiac readmissions. In contrast, high TIMI-score predicted cardiac mortality (HR 4.91 (1.92-12.58), p<0.001), as well as cardiac readmissions, both at 30-days (OR 7.76 (2.14-28.13), p<0.001)) and 12 months (OR 2.19 (1.01-4.72), p=0.044)). A higher proportion of patients on >1 antianginal agent suffered cardiac death during follow-up (HR 2.58 (1.11-6.00), p=0.029)), with a trend toward 12-month cardiac readmissions (OR 2.12 (0.96-4.69), p=0.063).
Conclusions: This study demonstrates that patients with medically managed surgical CAD who had an index ACS presentation, elevated TIMI risk score or require multiple antianginals are at high-risk of subsequent cardiac morbidity and mortality. Whether high risk invasive management has potential to mitigate this risk of mortality warrants further study.
Cailes, Benjamin
(
Austin Health
, Viewbank , Victoria , Australia )
D'amore, Matthew
(
Northern Health
, Melbourne , Victoria , Australia )
Koshy, Anoop
(
Austin Health
, Viewbank , Victoria , Australia )
Wettasinghe, Inun
(
Bendigo Health
, Bendigo , Victoria , Australia )
Dao, Thang
(
St Vincent's Hospital
, Melbourne , Victoria , Australia )
Yudi, Matias
(
Austin Health
, Melbourne , Queensland , Australia )
Yeoh, Julian
(
Austin Health
, Viewbank , Victoria , Australia )
Author Disclosures:
Benjamin Cailes:DO NOT have relevant financial relationships
| Matthew D'Amore:DO NOT have relevant financial relationships
| Anoop Koshy:No Answer
| Inun Wettasinghe:No Answer
| Thang Dao:DO NOT have relevant financial relationships
| Matias Yudi:No Answer
| Julian Yeoh:No Answer