A Machine Learning-Based Inflammatory Biomarker Panel Predicts Major Adverse Limb Events and Guides Precision Revascularization Strategy in Patients with Critical Limb-Threatening Ischemia
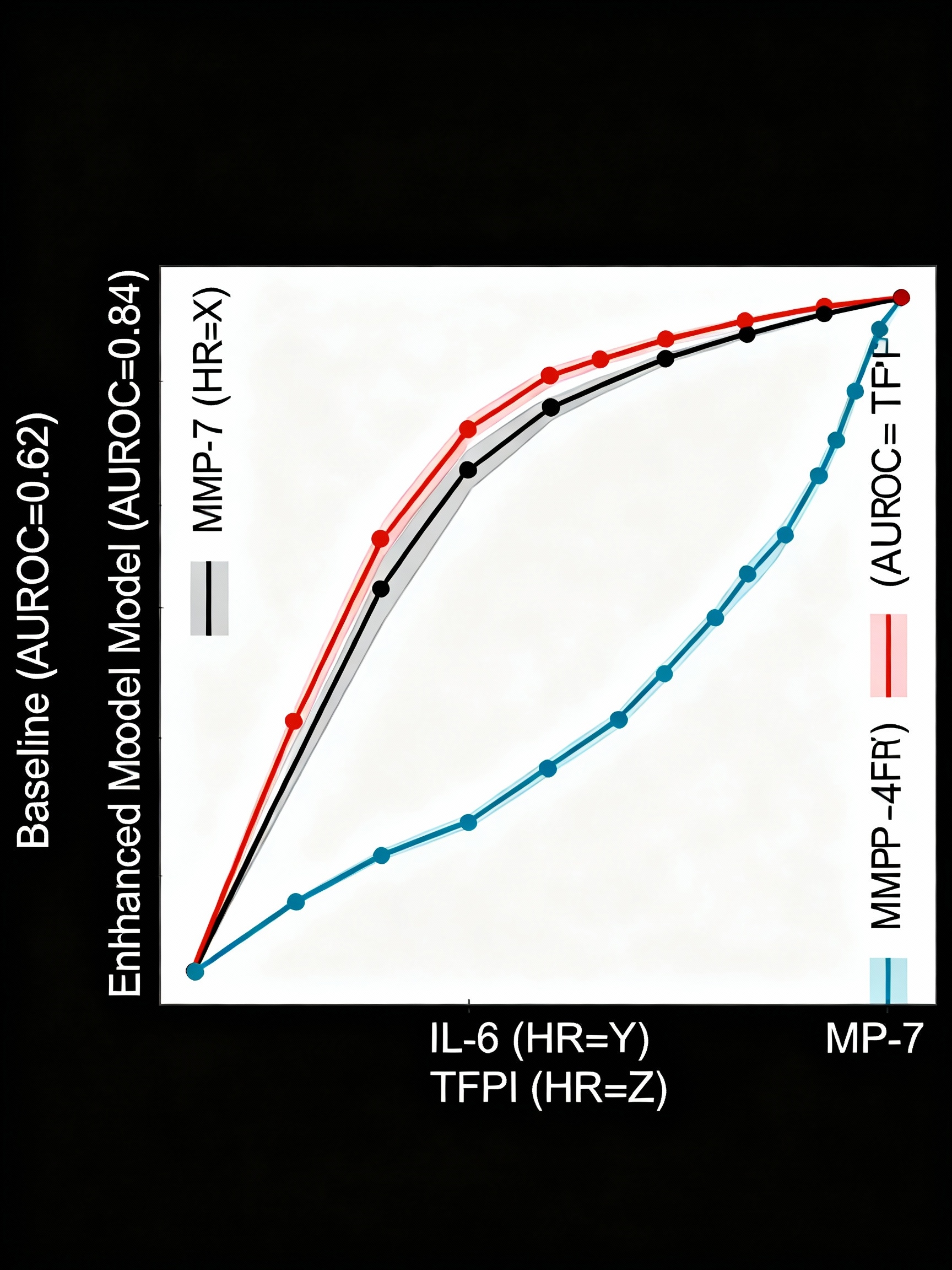
Abstract Body: Background: Critical limb-threatening ischemia (CLTI) is a leading cause of major amputation despite advances in revascularization, with 20-40% progressing to limb loss. Traditional prognostic systems (Rutherford, WIfI) lack precision identifying high-risk patients for major adverse limb events (MALE: amputation, repeat intervention, acute ischemia), limiting treatment personalization. Current risk stratification relies on clinical and anatomic variables without biologic markers of disease severity and amputation susceptibility. Hypothesis: Machine learning algorithms integrating clinical characteristics with targeted inflammatory biomarkers substantially improve MALE prediction and enable precision revascularization strategy selection in CLTI patients. Methods: Prospective multicenter study enrolled 847 consecutive CLTI patients from 18 vascular centers undergoing revascularization. Serum biomarkers (MMP-7, MMP-10, IL-6, CCL2, TFPI) quantified via multiplex immunoassay. Clinical variables: demographics, Rutherford, ankle-brachial index, transcutaneous oxygen pressure, WIfI stage, comorbidities, revascularization type. Primary outcome: 2-year MALE. Random forest machine learning model developed in discovery cohort (n=565, 67%) and validated in independent test cohort (n=282, 33%) using 10-fold cross-validation. Results: In validation cohort, MALE occurred in 156 of 282 patients (55.3%) at 2-year follow-up. Clinical variables predicted MALE with AUROC 0.62 (95% CI: 0.55-0.69). Biomarker panel improved accuracy to AUROC 0.84 (95% CI: 0.78-0.89), representing 36% improvement (p<0.001). Independent predictors: MMP-7 (HR 1.87, 95% CI: 1.31-2.67), IL-6 (HR 1.62, 95% CI: 1.14-2.31), low TFPI (HR 0.71, 95% CI: 0.51-0.97). Net reclassification improvement 0.44 (p<0.001). High-risk biomarker patients showed greater limb salvage with endovascular-first strategies versus low-burden patients (86.3% vs. 71.4%, p=0.012). Diabetic subgroup (n=312) demonstrated superior accuracy (AUROC 0.87, 95% CI: 0.81-0.93) versus non-diabetic (AUROC 0.79, 95% CI: 0.71-0.87). Conclusions: Machine learning biomarker integration substantially improves MALE prediction in CLTI, enabling precision-based treatment selection. Biomarker-guided approach identifies amputation-prone phenotypes benefiting from aggressive endovascular-first revascularization. Biomarker-stratified protocols could reduce amputation rates 15-20% nationally. Prospective randomized trial validation warranted.
Olvera Camacho, Fernando
(
Hospital General de Queretaro
, Queretaro , Queretaro , Mexico )
Orozco Zavala, Alondra
(
Mexican Social Security Institute
, Queretaro , Queretaro , Mexico )
Author Disclosures:
Fernando Olvera Camacho:DO NOT have relevant financial relationships
| Alondra Orozco zavala:No Answer