Symptomatic hemorrhage after thrombolysis: results from the Alteplase compared to Tenecteplase in patients with acute ischemic stroke trial
Abstract Body: Introduction: Because of the risk of infarcted tissue leading to symptomatic intracerebral hemorrhage (sICH) after intravenous thrombolysis for acute ischemic stroke, patients are monitored for at least 24 hours in a critical care setting. We aim to assess incidence and risk factors of sICH following thrombolysis for acute ischemic stroke. We hypothesize that the incidence of sICH is higher in patients with older age, longer symptom onset-to-needle (OTN), greater stroke severity, and lower baseline ASPECTS score.
Methods: Adults ≥18 years with acute ischemic stroke were randomized into the AcT trial to receive either intravenous TNK or tPA between December 2019 to January 2022 in 22 stroke centres in Canada. Patient demographics, stroke details, hemorrhagic complications (ICH, parenchymal hematoma, hemorrhagic infarct), and duration of hospital stay were collected. ANOVA and Chi-square tests compared demographic and clinical details across three groups: sICH, asymptomatic ICH (aICH), and no ICH (nICH). We developed logistic regression models to predict sICH and any ICH accounting for age, sex, pre-treatment NIHSS, OTN, baseline ASPECTS, and thrombolytic agent.
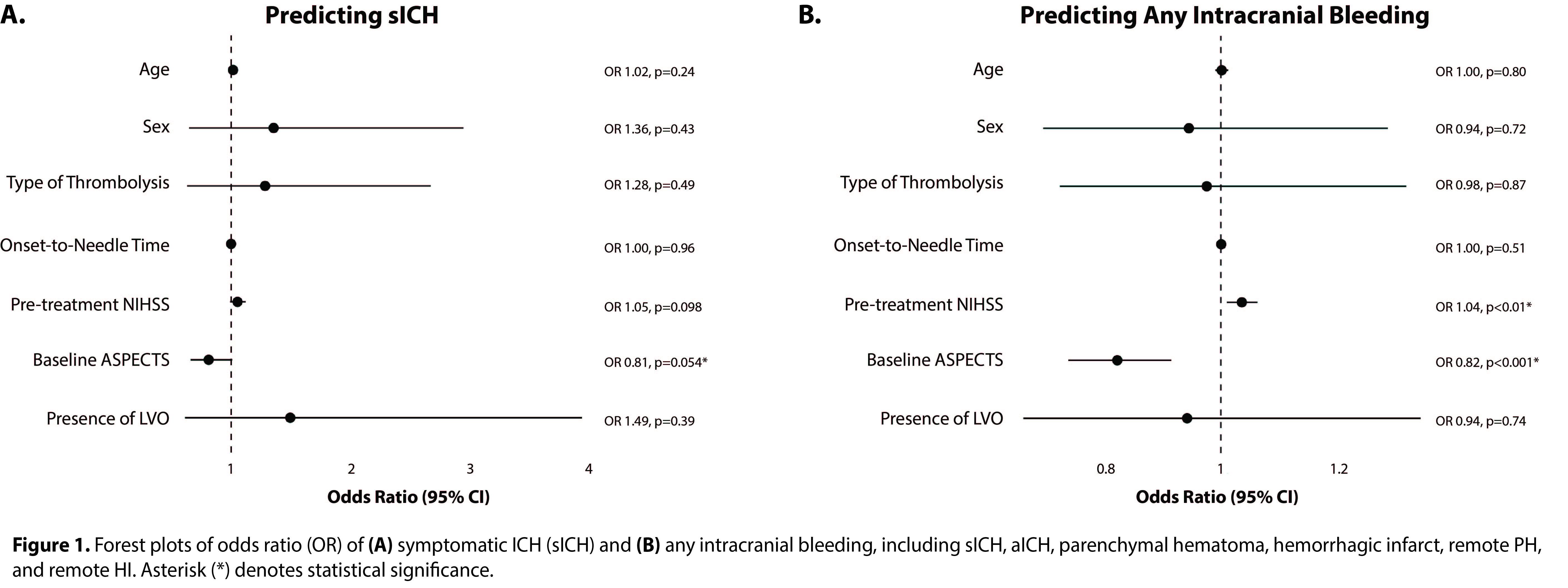
Preliminary Results: A total of 1556 participants were identified (sICH=51, aICH=261, nICH=1244). Mean age (72.02±14.2 years; p=0.11) and sex (48% female, p=0.13) were comparable between the groups. Mean pre-treatment NIHSS was highest in the sICH group (sICH 14.41±8.5, aICH 13.48±7.0, nICH 1055±6.6; p<0.001). Mean OTN was comparable across groups (sICH 141.90±62.6 min, aICH 142.65±65.1 min, nICH 144.46±69.5 min; p=0.90). Median ASPECTS was lower in the sICH group (sICH 8.00±1.7, aICH 9.00±1.6, nICH 9.00±1.4; p<0.001). There were higher odds of sICH with lower ASPECTS score (OR 0.81, 95% CI [0.66, 1], p=0.054). The risk of any intracranial hemorrhage was lower with higher ASPECTS score (OR 0.82, 95% CI [0.74, 0.91], p<0.001) and higher with worse NIHSS (OR 1.04, 95% CI [1.01, 1.06], p<0.01). Age, sex, OTN, and type of thrombolysis had no association with intracranial hemorrhage (Figure 1).
Conclusions: The risk of intracranial bleeding is greater when the infarct is more established and in patients with higher pre-treatment neurological deficit. Future analyses will seek to identify predictors of time to symptomatic bleeding, and to understand whether 24-hour ICU monitoring is needed for every recipient of thrombolysis.
Kuczynski, Andrea
(
University of Toronto
, Toronto , Ontario , Canada )
Sujanthan, Sajeevan
(
University of Toronto
, Toronto , Ontario , Canada )
Singh, Nishita
(
University of Manitoba
, Winnipeg , Manitoba , Canada )
Scales, Damon
(
Sunnybrook Health Sciences Centre
, Toronto , Ontario , Canada )
Adhikari, Neill
(
Sunnybrook Health Sciences Centre
, Toronto , Ontario , Canada )
Gladstone, David
(
University of Toronto
, Toronto , Ontario , Canada )
Demchuk, Andrew
(
University of Calgary
, Calgary , Alberta , Canada )
Menon, Bijoy
(
University of Calgary
, Calgary , Alberta , Canada )
Almekhlafi, Mohammed
(
University of Calgary
, Calgary , Alberta , Canada )
Swartz, Richard
(
SUNNYBROOK HSC
, Toronto , Ontario , Canada )
Author Disclosures:
Andrea Kuczynski:DO NOT have relevant financial relationships
| Mohammed Almekhlafi:DO NOT have relevant financial relationships
| Richard Swartz:No Answer
| Sajeevan Sujanthan:DO NOT have relevant financial relationships
| Nishita Singh:DO NOT have relevant financial relationships
| Damon Scales:No Answer
| Neill Adhikari:DO NOT have relevant financial relationships
| David Gladstone:No Answer
| Alexandre Poppe:DO have relevant financial relationships
;
Speaker:Roche Canada:Past (completed)
| Andrew Demchuk:DO NOT have relevant financial relationships
| Bijoy Menon:DO have relevant financial relationships
;
Individual Stocks/Stock Options:Circle CVI:Active (exists now)
; Advisor:Boehringer Ingelheim:Past (completed)