Age and Admission NIH Stroke Scale but Not Radiologic Collateral Status Predict Modified Rankin Score in Large and Medium Vessel Occlusion Ischemic Strokes
Abstract Body: Introduction: Neuroimaging is increasingly useful in predicting response to endovascular treatment (EVT) among acute ischemic stroke (AIS) patients. While radiologic collateral status is a known correlate of reperfusion and mortality in AIS patients with large vessel occlusions (LVOs) of the anterior circulation, whether this imaging marker is associated with patient functional status following EVT is unclear. Furthermore, the utility of collateral status in predicting outcomes of medium vessel occlusions (MeVOs), which account for 25-40% of AIS and are promising candidates for EVT, remains unknown. We evaluated the adjusted association of collateral status parameters with 90-day post-EVT functional outcomes in AIS patients with LVOs and MeVOs.
Methods: We retrospectively evaluated AIS patients treated at our institution between January 9, 2017, and January 10, 2023. The following inclusion criteria were applied: (i) CTA-confirmed anterior circulation large or medium vessel occlusion; (ii) diagnostic CT perfusion was performed; (iii) mechanical thrombectomy was performed. A low modified Rankin score (mRS) indicating good functional outcomes (i.e., functional independence) was defined as less than or equal to 2, in accordance with prior studies. Univariate and multivariate logistic regression analyses were conducted to determine associations between demographic, clinical, and radiologic factors and mRS ≤ 2.
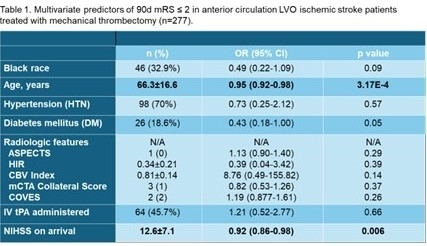
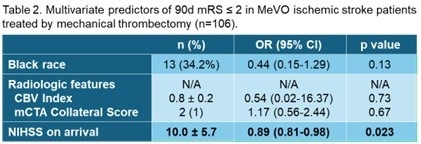
Results: A total of 277 LVO (mean age 66.3 ± 16.6, 57.0% female) and 106 MeVO (mean age 70.3 ± 13.9, 57.5% female) patients met inclusion criteria. On multivariate regression adjusted for race, age, sex, hypertension, diabetes mellitus, atrial fibrillation, radiologic features, IV alteplase administration, and admission NIHSS, young age (p = 0.0003) and low admission NIHSS (p = 0.006) were associated with good functional outcomes in LVO stroke (Table 1). Similarly, low admission NIHSS (p = 0.02) was associated with good functional outcomes in MeVO stroke (Table 2).
Conclusion: No significant association was detected between collateral status parameters — including single-phase CTA, multiphase CTA, and CT perfusion measures — and AIS functional outcomes following EVT in either LVO or MeVO strokes. Thus, although prior research suggests that good collateral status can predict successful reperfusion, collateral status parameters may be suboptimal for determining management of AIS in patients undergoing EVT where functional outcome is prioritized.
Srinivas, Tara
(
Johns Hopkins Medicine
, Baltimore , Maryland , United States )
Lakhani, Dhairya
(
Johns Hopkins Medicine
, Baltimore , Maryland , United States )
Balar, Aneri
(
West Virginia University
, Morgantown , West Virginia , United States )
Xu, Risheng
(
Johns Hopkins Medicine
, Baltimore , Maryland , United States )
Salim, Hamza
(
Johns Hopkins Medicine
, Baltimore , Maryland , United States )
Yedavalli, Vivek
(
Johns Hopkins School of Medicine
, Baltimore , Maryland , United States )
Author Disclosures:
Tara Srinivas:DO NOT have relevant financial relationships
| Dhairya Lakhani:No Answer
| Aneri Balar:DO NOT have relevant financial relationships
| Risheng Xu:DO NOT have relevant financial relationships
| Hamza Salim:No Answer
| Vivek Yedavalli:DO have relevant financial relationships
;
Consultant:RAPIDAI Ischemaview (Menlo Park, CA, USA):Active (exists now)