Distinguishing Intracerebral Hemorrhage from Acute Cerebral Ischemia in the Prehospital Setting: Development and Validation of the California Acute stroke Subtype PRehospital (CASPR) Scale
Abstract Body: Background: A prehospital, paramedic-administered scale to distinguish intracerebral hemorrhage (ICH) from acute cerebral ischemia (ACI) could improve routing to appropriate centers, enrich field randomized trials with targeted subtype patients, and potentially guide prehospital clinical treatment such as hyperacute blood pressure (BP) lowering. We aimed to create a quickly administered prehospital scale from prospectively performed field assessments.
Methods: Two scales were created from NIH Field Administration of Stroke Therapy Magnesium (FAST-MAG) trial data, using logistic regression model with backward stepwise variable selection and retention criterion of p<0.1. Scale one—CASPR-DB (Data-Based)—assessed 26 candidate variables available in routine prehospital care in 1675 patients (77.3% ACI, 22.7% ICH), who were randomly assigned to training (n=1114) or validation (n=561) sets. Scale two—CASPR-CS (Clinical Symptoms)—came from a subset of patients (n=467) in whom three additional clinical symptoms elicited in the field were also candidate items—headache, nausea, and progressing deficit.
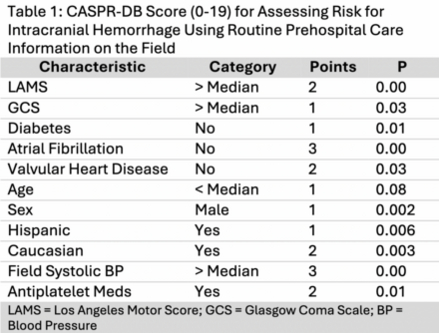
Results: For the CASPR-DB scale, the logistic regression model selected 10 of the 26 candidate variables in the training population. Factors associated with ICH were higher Los Angeles Motor Scale (LAMS) score, higher Glasgow Coma Score (GCS), higher systolic BP, Hispanic and Caucasian race-ethnicity, male sex, use of anti-platelet agents, decreased age, and absence of diabetes, atrial fibrillation, or valvular heart disease. Each was given a point value between 1-3, yielding a 19-point scale (Table 1).
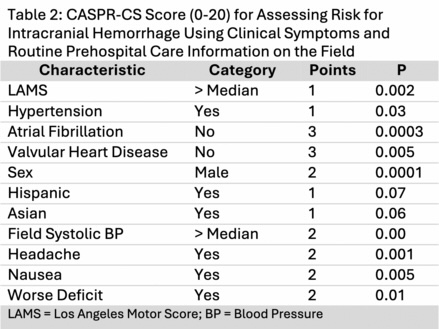
For the CASPR-CS scale, the logistic regression model selected 10 of the 29 candidate variables. All three symptom items—headache, nausea, and progressing deficit—were associated with ICH, along with 7 data-based variables. Each was given a point value between 1-3, yielding a 20-point scale (Table 2).
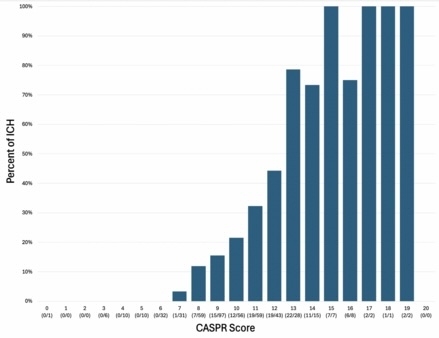
CASPR-DB performance in training was sensitivity 64.4%, specificity 78.6%, accuracy 71.5%, c=0.774 and in validation was sensitivity 69.3%, specificity 61.7%, accuracy 71.5%, c=0.710. CASPR-CS performance was sensitivity 71.8%, specificity 77.8%, accuracy 74.8%, c=0.830. Figure 1 shows the proportions of ICH patients at each CASPR-CS score level.
Conclusions: The CASPR-DB scale shows good and CASPR-CS scale very good performance in distinguishing ICH vs ACI in prehospital setting. These readily performable scales could improve prehospital routing and treatment of ICH patients.
Hsu, Jamie
(
University of California Los Angeles
, Los Angeles , California , United States )
Eckstein, Marc
(
University of Southern California
, Los Angeles , California , United States )
Stratton, Samuel
(
University of California Los Angeles
, Los Angeles , California , United States )
Liebeskind, David
(
University of California Los Angeles David Geffen School of Medicine
, Los Angeles , California , United States )
Sharma, Latisha
(
University of California Los Angeles David Geffen School of Medicine
, Los Angeles , California , United States )
Restrepo, Lucas
(
University of California Los Angeles David Geffen School of Medicine
, Los Angeles , California , United States )
Kim-tenser, May
(
University of Southern California
, Los Angeles , California , United States )
Valdes-sueiras, Miguel
(
University of California Los Angeles David Geffen School of Medicine
, Los Angeles , California , United States )
Gornbein, Jeffrey
(
UCLA
, Los Angeles , California , United States )
Hamilton, Scott
(
Stanford University
, Palo Alto , California , United States )
Conwit, Robin
(
NINDS
, Lutherville , Maryland , United States )
Taleb, Shayandokht
(
Kaiser Permanente
, Los Angeles , California , United States )
Sung, Gene
(
University of Southern California
, Los Angeles , California , United States )
Saver, Jeffrey
(
University of California Los Angeles David Geffen School of Medicine
, Los Angeles , California , United States )
Sanossian, Nerses
(
University of Southern California
, Los Angeles , California , United States )
Author Disclosures:
Jamie Hsu:DO NOT have relevant financial relationships
| Scott Hamilton:No Answer
| Robin Conwit:DO NOT have relevant financial relationships
| Shayandokht Taleb:DO NOT have relevant financial relationships
| Gene Sung:DO NOT have relevant financial relationships
| Jeffrey Saver:DO have relevant financial relationships
;
Consultant:Abbott:Active (exists now)
; Individual Stocks/Stock Options:Viz.ai:Active (exists now)
; Individual Stocks/Stock Options:Let's Get Proof:Active (exists now)
; Individual Stocks/Stock Options:Neuronics:Active (exists now)
; Consultant:Genentech:Expected (by end of conference)
; Consultant:Roche:Active (exists now)
; Consultant:Novo Nordisc:Active (exists now)
; Consultant:AstraZeneca:Active (exists now)
; Consultant:BrainQ:Active (exists now)
; Consultant:Medtronic:Active (exists now)
| Nerses Sanossian:No Answer
| Marc Eckstein:No Answer
| Samuel Stratton:DO NOT have relevant financial relationships
| David Liebeskind:DO NOT have relevant financial relationships
| Latisha Sharma:DO NOT have relevant financial relationships
| Lucas Restrepo:No Answer
| May Kim-Tenser:DO NOT have relevant financial relationships
| miguel valdes-sueiras:No Answer
| Jeffrey Gornbein:DO NOT have relevant financial relationships