Small Vessel Disease is Associated With Primary Aldosteronism in Acute Ischemic Stroke
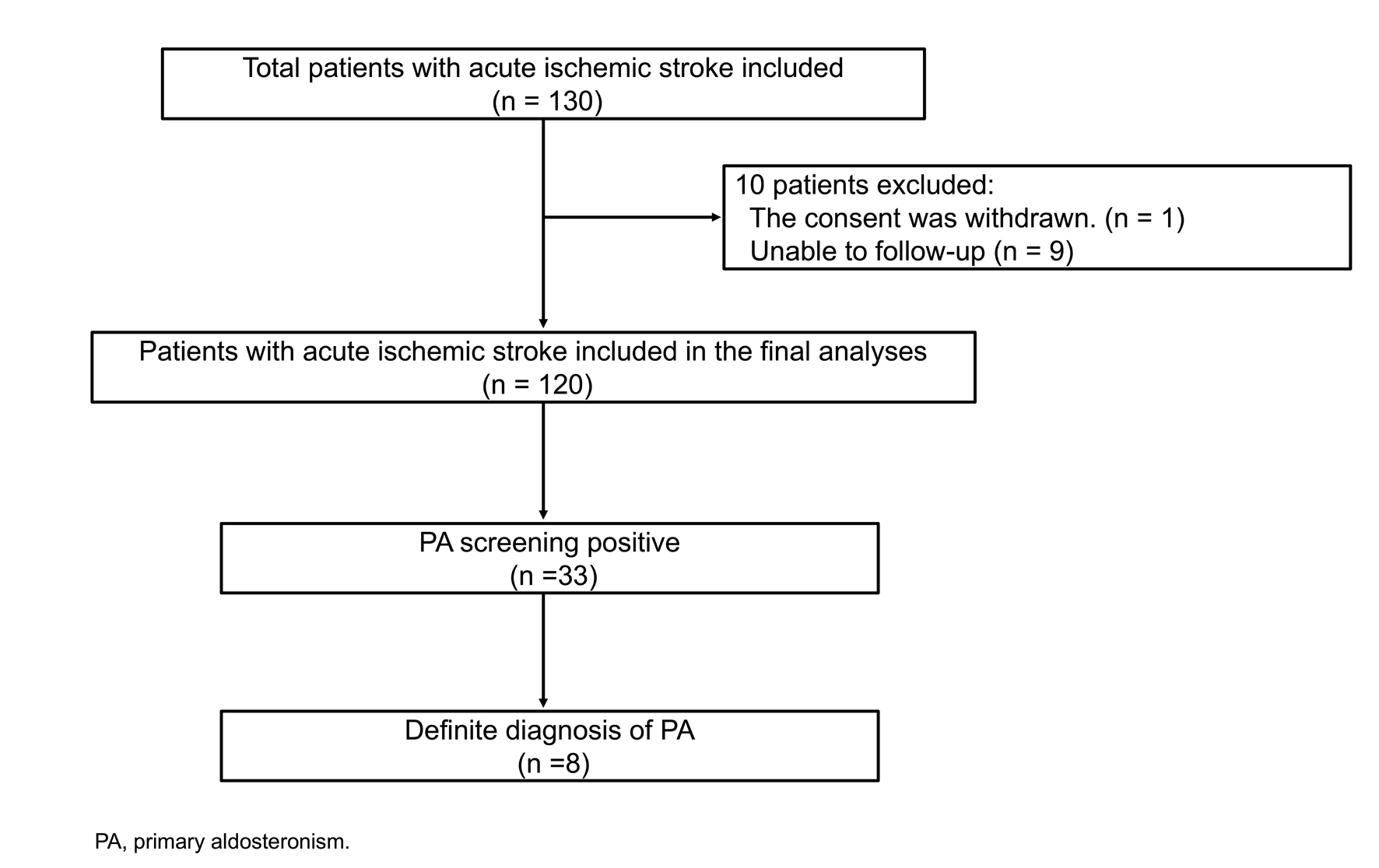
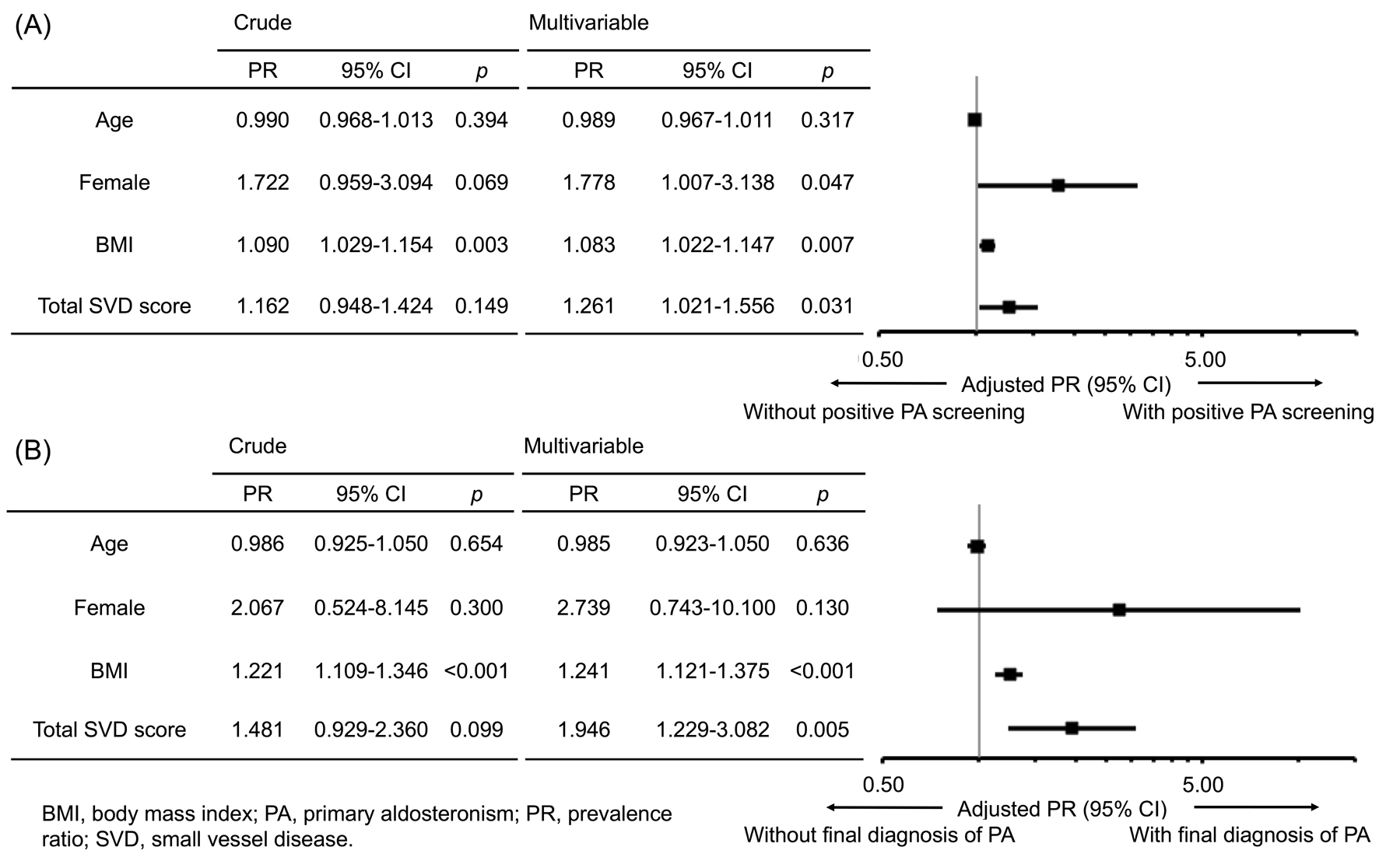
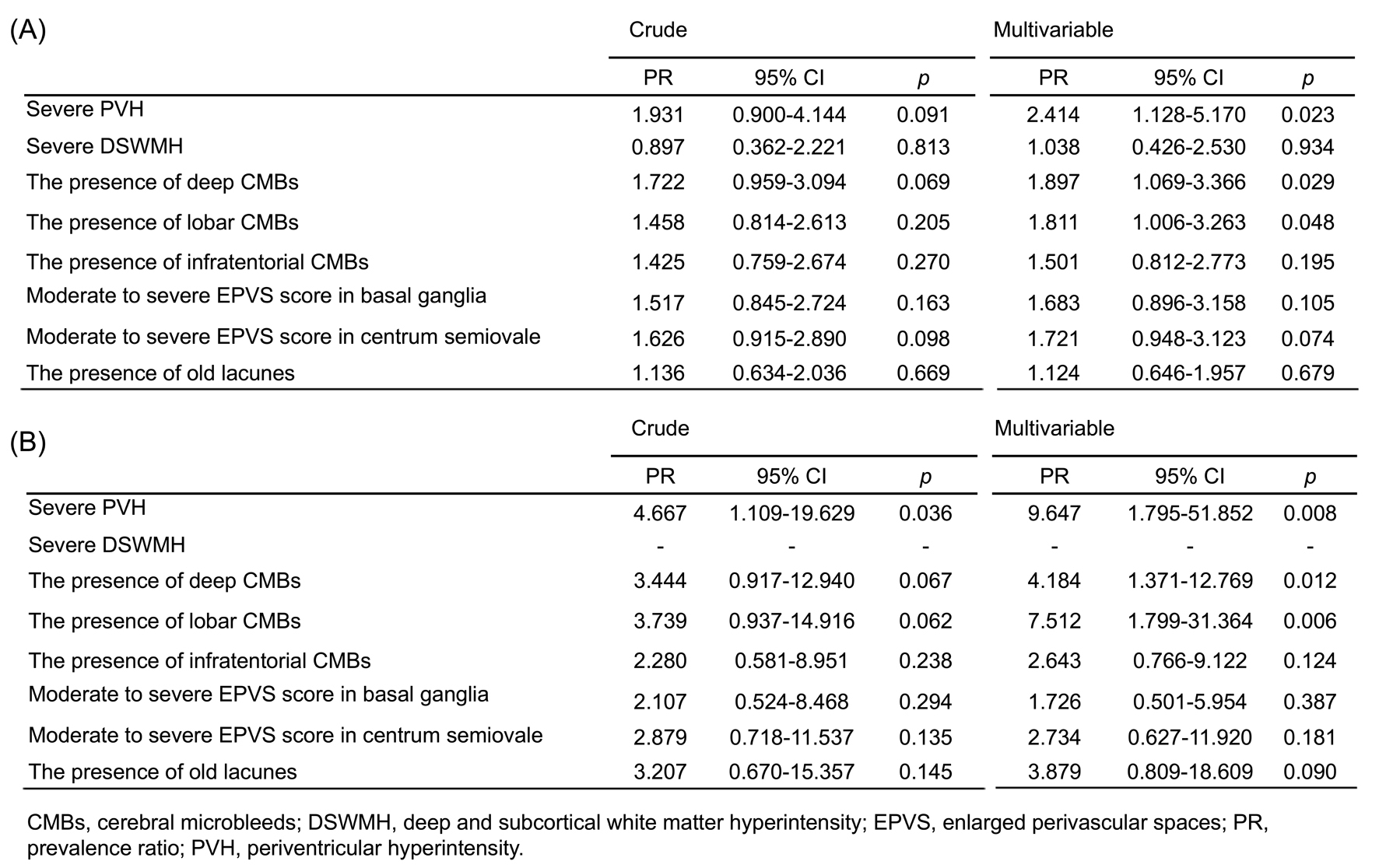
Abstract Body: Background and Purpose: Primary aldosteronism (PA) is characterized by the autonomous overproduction of aldosterone leading to the risk of occurrence of acute ischemic stroke (AIS), but the exact prevalence of PA is unknown in patients with AIS. PA induces oxidative stress and inflammation through vascular endothelial cells, which may damage small vessel disease (SVD). We conducted a prospective study to investigate the prevalence of screening and definite diagnosis of PA in patients with AIS. Next, we aimed to reveal whether SVD markers could be associated with PA. Methods: We screened consecutive patients with AIS who participated in our prospective study to investigate the prevalence of PA and followed up for PA evaluation from October 2020 to December 2022. Inclusion criteria were patients with AIS hospitalized and diagnosed with hypertension. Exclusion criteria were patients taking medications affecting renin, aldosterone, and catecholamines. The screening criteria for PA was defined as the aldosterone-to-renin ratio > 200. Final diagnosis of PA was judged by endocrinologist if one of the captopril challenge test, saline infusion test, and furosemide-upright test was positive following discharge. We evaluated total SVD score based on white matter hyperintensities (separately scored by periventricular hyperintensity [PVH] and deep and subcortical white matter hyperintensity), cerebral microbleeds (CMBs; categorized into deep, lobar, and infratentorial lesions), enlarged perivascular spaces (separately scored in basal ganglia and centrum semiovale), and old lacunes on MRI. Results: We included 120 patients with AIS (93 [78%] male, median age 62 years, Figure 1). The screening for PA was positive in 33 (28%) patients and 8 (7%) patients were finally diagnosed with definite PA. In Poisson regression analysis with a robust variance estimator, total SVD score was related to positive PA screening (prevalence ratio [PR] 1.261, 95% CI 1.021-1.556, p = 0.031) and definite PA diagnosis (PR 1.946, 95% CI 1.229-3.082, p = 0.005, Figure 2). In terms of each SVD marker, severe PVH, and deep and lobar CMBs were associated with positive PA screening and definite PA diagnosis (Figure 3). Conclusions: Twenty-eight percent of patients with AIS were positive for PA screening, and then about a quarter of them were confirmed as definite PA. SVD burden, especially PVH, and deep and lobar CMBs, might be associated with positive screening and definite diagnosis of PA.
Okumura, Motohiro
(
The Jikei University School of Medicine
, Tokyo , Japan )
Sato, Takeo
(
The Jikei University School of Medicine
, Tokyo , Japan )
Tsujimoto, Yuki
(
The Jikei University School of Medicine
, Tokyo , Japan )
Yamashiro, Kenji
(
The Jikei University School of Medicine
, Tokyo , Japan )
Watanabe, Yui
(
The Jikei University School of Medicine
, Tokyo , Japan )
Kida, Hiroyuki
(
The Jikei University School of Medicine
, Tokyo , Japan )
Nakada, Ryoji
(
The Jikei University Kashiwa Hospital
, Kashiwa-shi , Japan )
Kitagawa, Tomomichi
(
The Jikei University School of Medicine
, Tokyo , Japan )
Takatsu, Hiroki
(
The Jikei University School of Medicine
, Tokyo , Japan )
Komatsu, Teppei
(
The Jikei University School of Medicine
, Tokyo , Japan )
Sakuta, Kenichi
(
The Jikei University School of Medicine
, Tokyo , Japan )
Sakai, Kenichiro
(
The Jikei University School of Medicine
, Tokyo , Japan )
Mitsumura, Hidetaka
(
The Jikei University School of Medicine
, Tokyo , Japan )
Nishimura, Rimei
(
The Jikei University School of Medicine
, Tokyo , Japan )
Iguchi, Yasuyuki
(
The Jikei University School of Medicine
, Tokyo , Japan )
Author Disclosures:
Motohiro Okumura:DO NOT have relevant financial relationships
| Teppei Komatsu:DO NOT have relevant financial relationships
| Kenichi Sakuta:DO NOT have relevant financial relationships
| Kenichiro Sakai:DO NOT have relevant financial relationships
| Hidetaka Mitsumura:DO NOT have relevant financial relationships
| Rimei Nishimura:DO have relevant financial relationships
;
Speaker:Sanofi Co., Ltd:Active (exists now)
; Research Funding (PI or named investigator):Arkley:Active (exists now)
; Research Funding (PI or named investigator):KOWA:Active (exists now)
; Consultant:Medtronic Co., Ltd:Active (exists now)
; Consultant:Abbott:Active (exists now)
; Consultant:Novo Nordisk Pharma Co., Ltd:Active (exists now)
; Consultant:Eli Lilly Japan Co., Ltd:Active (exists now)
; Speaker:Teijin:Active (exists now)
; Speaker:Nippon Boehringer Ingelheim Co., Ltd:Active (exists now)
| Yasuyuki Iguchi:DO have relevant financial relationships
;
Speaker:Daiichi-Sankyo:Active (exists now)
; Speaker:Alexion:Active (exists now)
; Speaker:Amagen Biogen:Active (exists now)
; Speaker:Takeda:Active (exists now)
; Speaker:Sumitomo Dainippon:Active (exists now)
; Speaker:Pfizer:Active (exists now)
; Speaker:Otsuka:Active (exists now)
; Speaker:Novartis:Active (exists now)
; Speaker:Mitsubishi-Tanabe:Active (exists now)
; Speaker:JB:Active (exists now)
; Speaker:Eisai:Active (exists now)
; Speaker:CSL-Behring:Active (exists now)
; Speaker:Chugai:Active (exists now)
| Takeo Sato:DO NOT have relevant financial relationships
| Yuki Tsujimoto:DO NOT have relevant financial relationships
| Kenji Yamashiro:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Teijin Pharma Ltd.:Past (completed)
; Research Funding (PI or named investigator):Ono Pharmaceutical Co., Ltd.:Past (completed)
| Yui Watanabe:DO NOT have relevant financial relationships
| Hiroyuki Kida:DO NOT have relevant financial relationships
| Ryoji Nakada:DO NOT have relevant financial relationships
| Tomomichi Kitagawa:DO NOT have relevant financial relationships
| Hiroki Takatsu:DO NOT have relevant financial relationships