Endovascular thrombectomy plus intravenous thrombolysis versus endovascular thrombectomy alone in patients with large core infarct
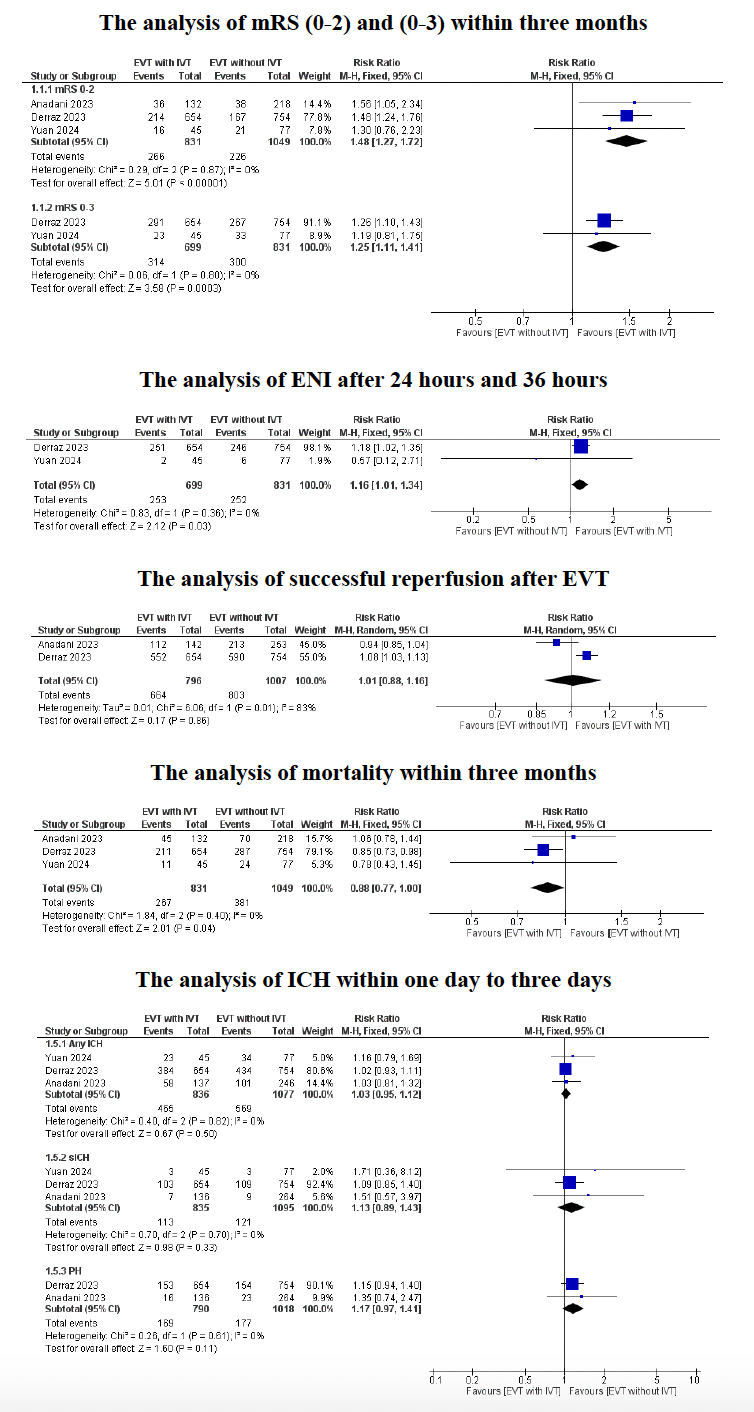
Abstract Body: Background: For patients meeting eligibility criteria, endovascular thrombectomy (EVT) remains the gold standard treatment for acute ischemic stroke (AIS) caused by large vessel occlusion (LVO). A few randomized trials have investigated EVT in AIS-LVO with large ischemic infarcts (LII). We studied the impact of intravenous thrombolysis (IVT) on the outcomes of EVT in those patients. Methods: We conducted a meta-analysis using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist and the Cochrane Handbook of Systematic Reviews and Interventions. We searched 4 databases (PubMed, Scopus, Web of Science, and Cochrane CENTRAL) from inception till June 11, 2024. We performed our analysis with RevMan utilizing a pooled risk ratio (RR) with a 95% confidence interval (CI). Results: Three studies with a total of 1,927 patients investigated EVT with and without IVT in AIS-LVO patients with LII. All 3 studies reported on modified Rankin Scale (mRS) score of 0-2 at 3 months, (831 patients in the EVT+IVT group and 1,049 patients in the EVT-only group), with a statistically significant difference favoring EVT+IVT (RR: 1.48, 95%CI: 1.27, 1.72, P< 0.00001). Two studies reported on mRS score of 0-3 (699 patients in the EVT+IVT group and 831 patients in the EVT-only group). The analysis also favored EVT+IVT (RR: 1.25, 95%CI: 1.11, 1.41, P= 0.0003). Two studies reported on early neurological improvement (ENI) after 24 and 36 hours (699 patients in the EVT+IVT group and 831 patients in the EVT-only group). The analysis revealed a statistically significant difference favoring EVT+IVT (RR: 1.16, 95%CI: 1.01, 1.34, P= 0.03). Two studies reported on successful reperfusion after EVT with no statistically significant difference between the two groups (RR: 1.01, 95%CI: 0.88, 1.16, P= 0.86). All 3 studies reported on mortality (831 patients in the EVT+IVT group and 1,049 patients in the EVT-only group), and the analysis favored EVT+IVT (RR: 0.88, 95%CI: 0.77, 1, P= 0.04). Lastly, our subgroup analysis did not favor any of the two groups across different types of intracranial hemorrhage (ICH). Conclusion: Our results indicate a beneficial impact of IVT on the clinical outcomes of EVT in AIS-LVO patients with LII regarding functional outcomes and early neurological improvement. IVT was also associated with a lower mortality rate but not with an increased risk of ICH. More studies of larger sample sizes are needed to corroborate such results.
Elfil, Mohamed
(
University of Miami/Jackson Health System
, Miami , Florida , United States )
Abbas, Abdallah
(
Al-Azhar University
, Damietta , Egypt )
Fountain, Hayes
(
University of Miami
, Miami , Florida , United States )
Abdul-hamid, Ebrahem
(
Al-Azhar University
, Damietta , Egypt )
Aladawi, Mohammad
(
University of Alabama Medical Cent
, Birmingham , Alabama , United States )
Najdawi, Zaid
(
University of Nebraska Medical Center
, Omaha , Nebraska , United States )
Elmashad, Ahmed
(
Westchester Medical Center
, Valhalla , New York , United States )
Ghaith, Hazem
(
Al-Azhar University
, Cairo , Egypt )
Dawod, Giana
(
Weill Cornell Medical Center
, Manhattan , New York , United States )
Malik, Amer
(
University of Miami/Jackson Health System
, Miami , Florida , United States )
Al-mufti, Fawaz
(
Westchester Medical Center
, Valhalla , New York , United States )
Author Disclosures:
Mohamed Elfil:DO NOT have relevant financial relationships
| Amer Malik:DO NOT have relevant financial relationships
| Fawaz Al-Mufti:No Answer
| Abdallah Abbas:No Answer
| Hayes Fountain:DO NOT have relevant financial relationships
| Ebrahem Abdul-Hamid:No Answer
| Mohammad Aladawi:DO NOT have relevant financial relationships
| Zaid Najdawi:DO NOT have relevant financial relationships
| Ahmed Elmashad:DO NOT have relevant financial relationships
| Hazem Ghaith:DO NOT have relevant financial relationships
| Giana Dawod:No Answer