Place of Death for Cerebrovascular Mortality, 2018–2023: Hospice–Forward U.S. Trends From CDC WONDER
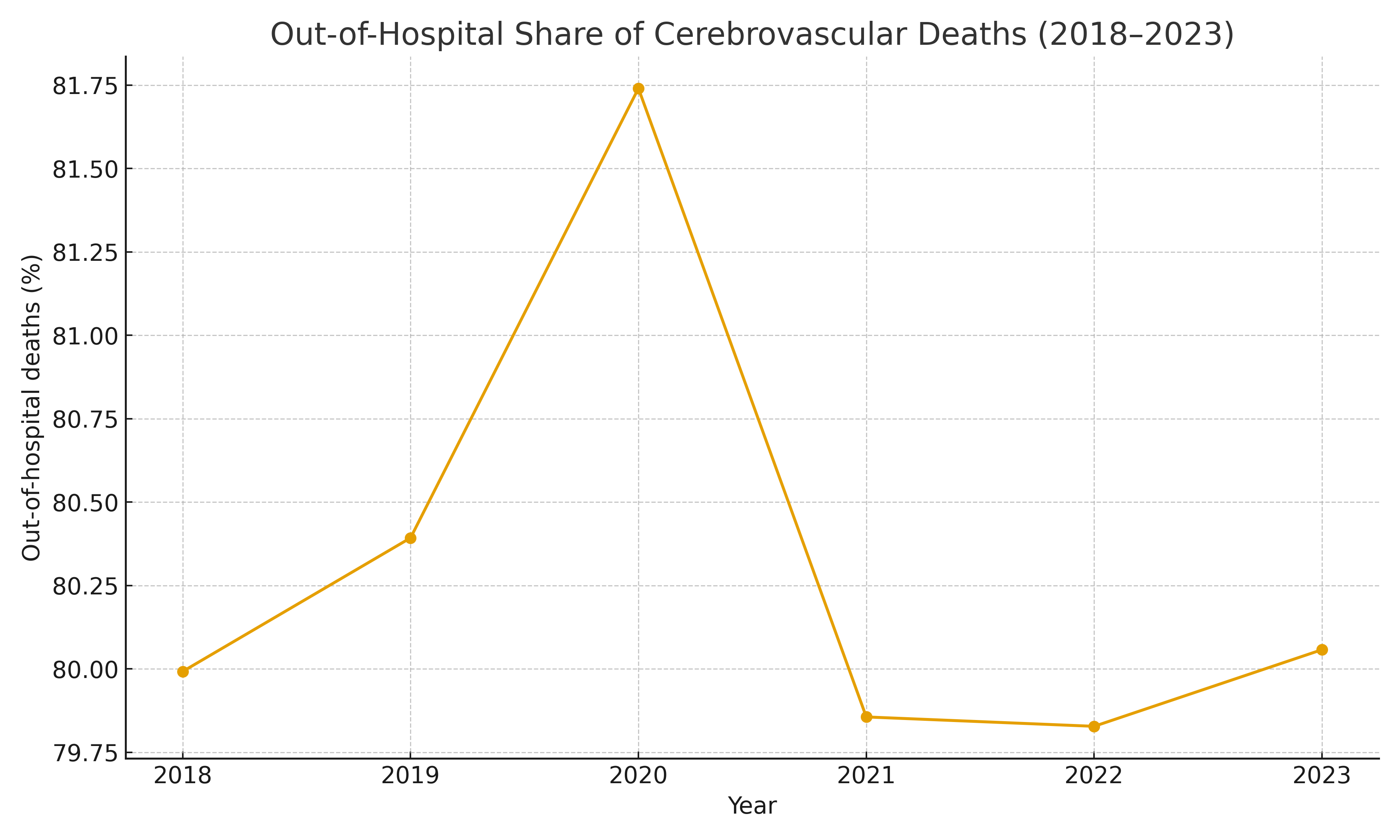
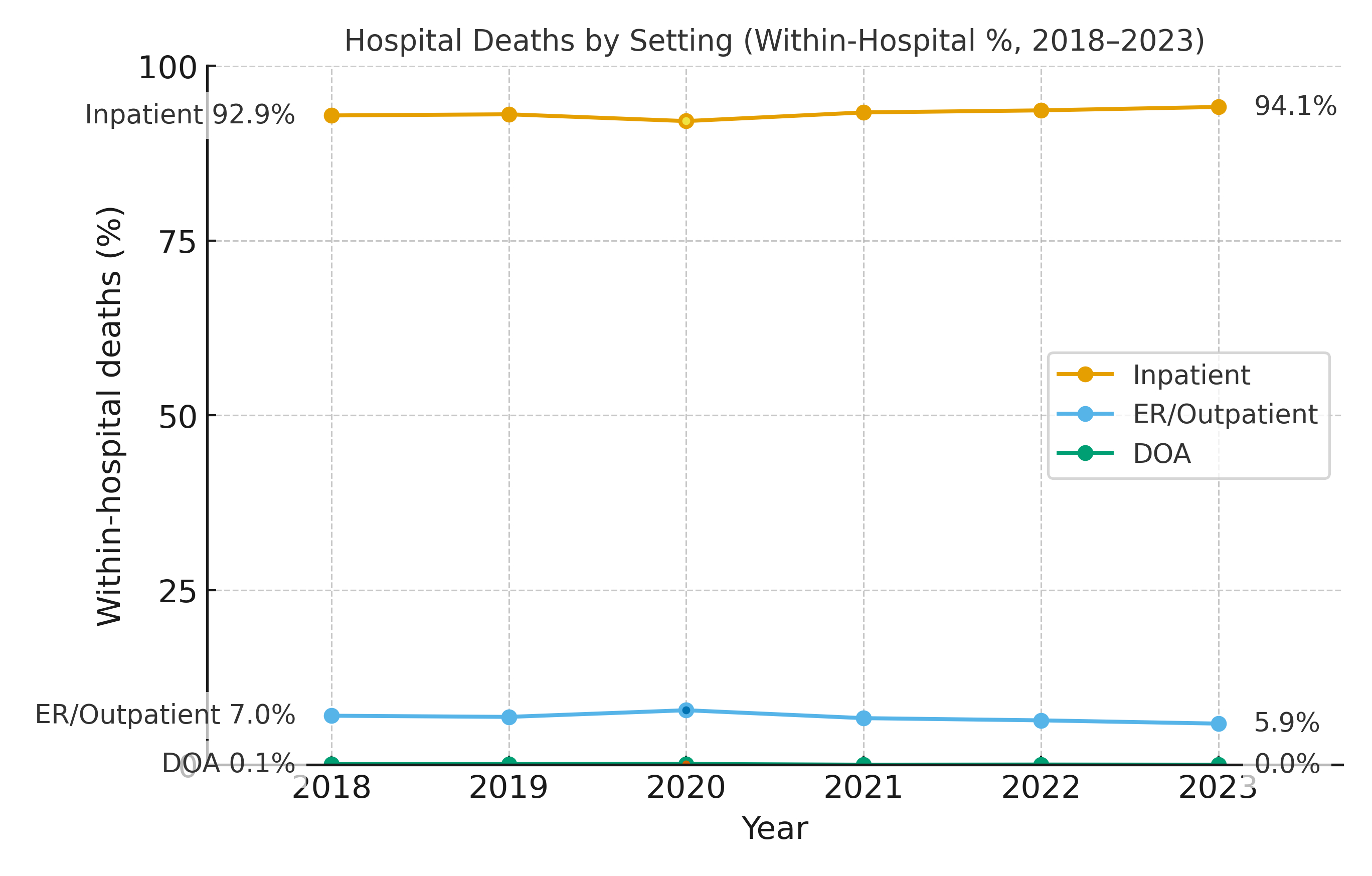
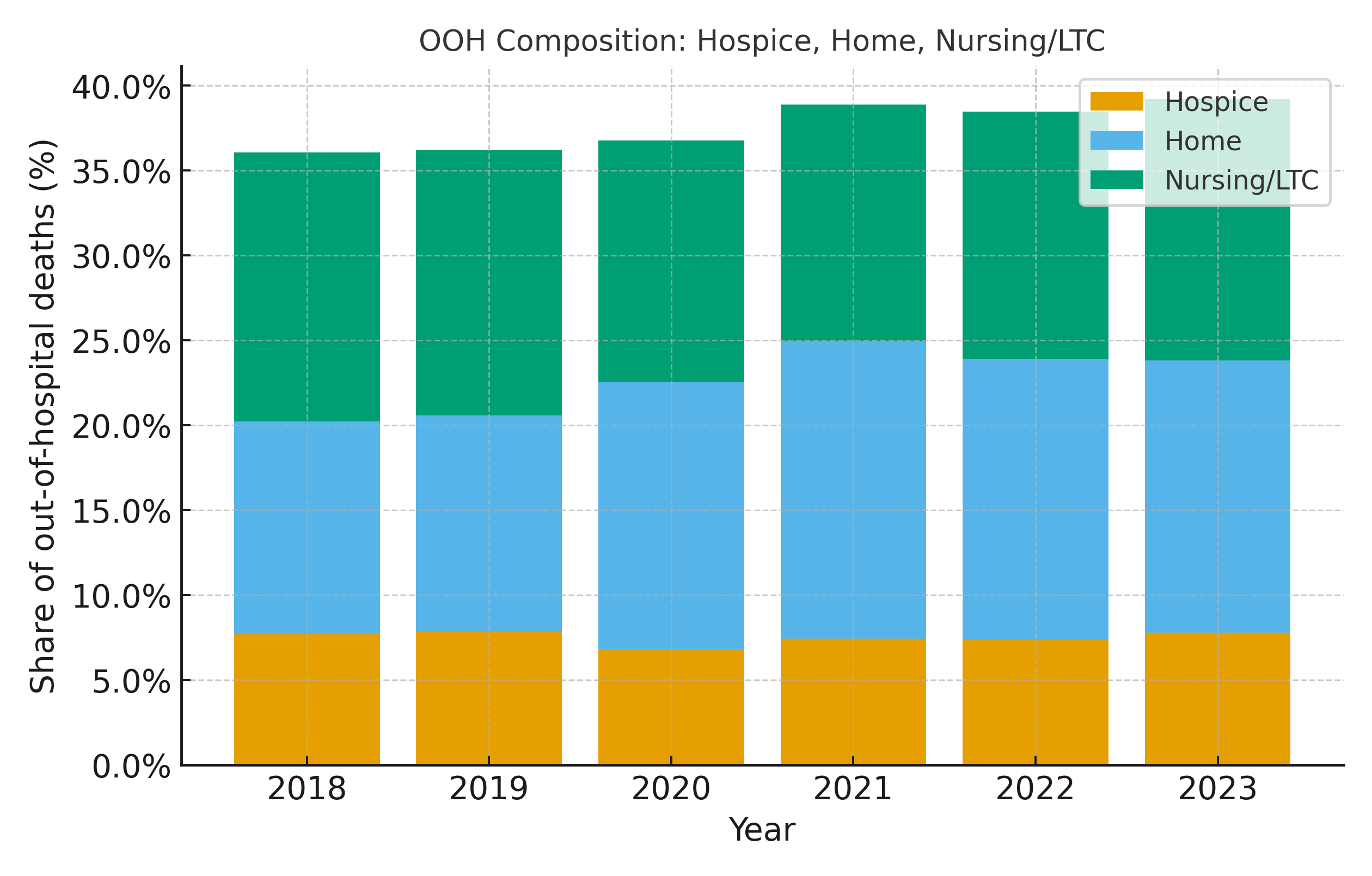
Abstract Body: Background Where cerebrovascular deaths occur reflects emergency access, end-of-life preferences, and palliative capacity. Whether hospice’s role changed during and after the pandemic is unclear. Hypothesis Out-of-hospital (OOH) deaths rose in 2020 and stabilized thereafter; hospice’s share within OOH would not expand meaningfully post-2020. Methods CDC WONDER Multiple Cause of Death (final, 2018–2023; I60–I69). Place of death was grouped as hospital (inpatient, emergency/outpatient, dead-on-arrival [DOA]) vs OOH (home, hospice facility, nursing/long-term care [LTC], other/unspecified). We computed annual counts, OOH share, and OOH composition (hospice, home, LTC). For adjustment, a binomial GLM (logit link) modeled OOH/(total) by Year, Sex, Race (Single-Race-6), Education with frequency weights; marginal year predictions were averaged by observed stratum totals. We explored small-cell instability with Beta–Binomial empirical-Bayes (EB) for Race×Year; subgroup cross-tabs were suppression-limited in U.S. totals. Results There were 1,775,960 cerebrovascular deaths (2018–2023). OOH share was 80.0% (2018), 81.7% (2020 peak), 80.1% (2023); adjusted estimates closely matched crude (2018–2023 adj. range: 79.9%–81.7%), indicating trends were not explained by demographic shifts. Within OOH, hospice’s share was stable: 7.7% (2018), 6.8% (2020), 7.8% (2023); era means pre 2018–2019 vs post 2021–2023 were 7.7% vs 7.5% of OOH and 6.2% vs 6.0% of all deaths. By contrast, home deaths comprised a rising fraction of OOH (12.5% → 16.0%; era means 12.6% → 16.7%), while LTC was flat to slightly lower (15.8% → 15.4%; era means 15.7% → 14.6%). In hospitals, the mix shifted toward inpatient (92.9%→94.1%) and away from ER/outpatient (7.0%→5.9%); DOA ~0–0.1%. EB did not alter national conclusions given suppression in subgroup cross-tabs. Conclusions Cerebrovascular deaths remain predominantly out-of-hospital (~80%) with a 2020 peak and stabilization thereafter. Hospice’s proportional role did not expand post-pandemic, while home deaths grew within the OOH mix. These findings suggest sustained reliance on community/residential settings without compensatory growth in facility-based hospice. Strengthening early palliative engagement, equitable hospice referral pathways, and community stroke preparedness—paired with monitoring of place-of-death indicators—may better align preferences, capacity, and system performance in the post-COVID era.
Tran, Tam
(
Washington University School of Medicine
, Saint Louis , Missouri , United States )
Lee, Wei Jun
(
SUNY Downstate Health Sciences University
, Brooklyn , New York , United States )
Nguyen, Dang
(
Harvard University
, Cambridge , Massachusetts , United States )
Marzouk, Sammer
(
Northwestern Feinberg School of Medicine
, Chicago , Illinois , United States )
Le, Trang
(
Cardiovascular Research, Methodist
, Brooklyn , New York , United States )
Truong, Hieu
(
Prime Saint Francis Hospital
, Evanston , Illinois , United States )
Erkelens, Bryce
(
University of Southern California
, Los Angeles , California , United States )
Huynh, Han
(
ollege of Medical Science and Technology - Taipei Medical University
, Taipei , Taiwan )
Le, Minh
(
Cardiovascular Research, Methodist
, Brooklyn , New York , United States )