Healthcare Interactions, Diagnoses, and Service Utilization Preceding Cardiovascular Mortality Associated with Homelessness
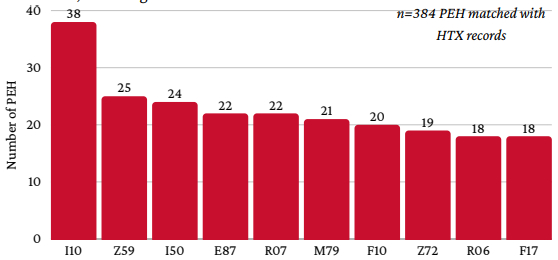
Abstract Body: Background: Cardiovascular disease (CVD) persists as the leading cause of death among U.S. adults. Persons experiencing homelessness (PEH) face a disproportionate burden with earlier onset and premature mortality. The average age of CVD death among PEH is 58–62 years, while 83% of CVD deaths occur after 65 in the general population. This disparity reflects combined effects of traditional risk factors, housing instability, barriers to care, and structural inequity. It is hoped that examining healthcare and service interactions and diagnostic patterns preceding CVD death may inform interventions to reduce PEH mortality. Methods: This study analyzed medicolegal records of PEH deaths reported by a large urban county medical examiner between 2021-2024. Decedent data from 2021-2023 were linked with a community-based (PCIC; n=199) and health information exchange (HTX; n=384) to evaluate temporal trends in healthcare, service utilization, comorbidities, social determinants, and clinical factors preceding death. Results: From 2021-2024, CVD accounted for 29.1%, 29.8%, 28.9%, and 26.9% of PEH deaths. Healthcare and service use increased near-exponentially in the months before death across EMS, clinics, hospitals, social services, and law enforcement. In the year before death, circulatory system disease (CSD) was the second most common diagnosis in PCIC (n=57) and third in HTX (n=138). Excluding F and Z codes, PCIC commonly recorded pain not elsewhere classified (G89; n=41) and hypertension (HTN) (I10; n=30); HTX included HTN (n=84), and CVD-related conditions such as heart failure (I50; n=42), abnormal breathing (R06; n=50), and respiratory failure (J96; n=45). Including F and Z codes, frequent diagnoses were HTN (n=38), housing instability (Z59; n=25), heart failure (n=24), electrolyte imbalance (E87; n=22), and chest/throat pain (R07; n=22). Conclusion: Stable CVD mortality among PEH reflects an ongoing burden. CSD consistently ranked among the top diagnoses preceding death, with pain, HTN, heart failure, abnormal breathing, and respiratory failure observed as contributors to CVD morbidity and mortality. Housing instability was commonly, but not universally documented, underscoring the need for integrated medical and social interventions. Rising service utilization before death suggests crisis-driven care. Strengthening coordination, care continuity, and community-based interventions may enable early detection and management of CVD, reducing preventable deaths.
King, Ben
(
University of Houston, COM
, Houston , Texas , United States )
Swamy, Shriya
(
University of Houston, COM
, Houston , Texas , United States )
Lin, Lucas
(
University of Houston, COM
, Houston , Texas , United States )
Stratemann, Carlie
(
University of Houston, COM
, Houston , Texas , United States )
Kazmi, Mahvish
(
University of Houston, COM
, Houston , Texas , United States )
Buck, David
(
University of Houston
, Houston , Texas , United States )