Health Care Access and the Hypertension Care Cascade Among Adults With Hypertension in NHANES 2021–2023
Abstract Body: Background: Hypertension remains a leading cardiovascular risk factor, yet gaps in care persist. The hypertension care cascade (awareness, treatment, control) offers a framework for identifying intervention points. Examining its association with healthcare access can inform strategies to improve control. We quantified progression through the cascade and evaluated associations with healthcare access among adults with hypertension.
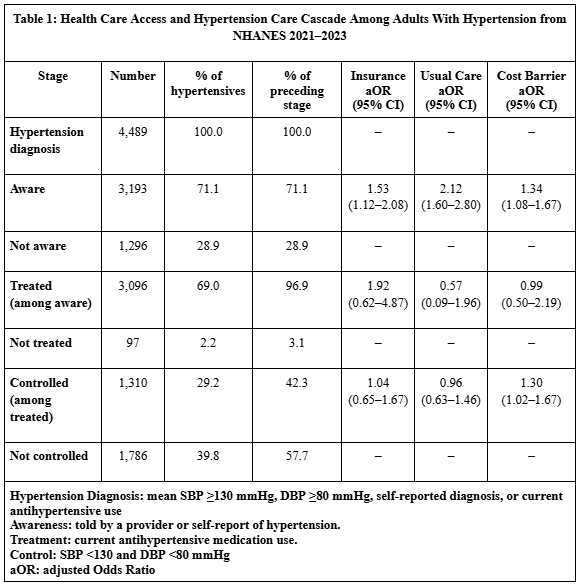
Methods: We analyzed adults ≥18 years with hypertension (N=4,489) in NHANES 2021–2023. Hypertension was defined as mean systolic blood pressure (SBP) ≥130 mmHg, diastolic blood pressure (DBP) ≥80 mmHg, self-reported diagnosis, or current antihypertensive use. Awareness was defined as being told by a provider or self-report; treatment as self-reported antihypertensive use; and control as SBP <130 and DBP <80 mmHg. Healthcare access indicators included insurance coverage, usual source of care, and cost-related barriers (yes vs no for each). Logistic regression models adjusted for age, sex, race/ethnicity, education, and income-to-poverty ratio. Because this NHANES cycle excluded prescription medication data, treatment relied on self-report and may be underestimated.
Results: The mean age was 58.8±16.0 years (95% CI: 58.3–59.2); 47.4% were male. Among adults with hypertension, 71.1% were aware, 69.0% were treated, and 29.2% achieved control (42.3% of those treated). Awareness was higher among those with insurance (aOR 1.53, 95% CI 1.12–2.08), a usual source of care (aOR 2.12, 1.60–2.80), and cost barriers (aOR 1.34, 1.08–1.67). Treatment was associated with female sex (aOR 2.46, 1.53–4.02) and higher income (aOR 1.21, 1.02–1.44) but not significantly with access measures (p>0.05). Control was more likely among those with higher education (aOR 1.11, 1.02–1.21) and cost barriers (aOR 1.30, 1.02–1.67) but was not associated with insurance or usual source of care. (Table 1)
Conclusion: Fewer than one in three U.S. adults with hypertension achieved control. Insurance and a usual source of care were strongly associated with awareness, underscoring the importance of consistent access. The positive association between cost barriers and control may reflect reverse causation, where those who actively seek healthcare and achieve targets report cost barriers. Strengthening affordability and continuity of care remains vital to improving hypertension management and cardiovascular health.