Opportunistic Screening versus Population-Wide for Hypertension: A Microsimulation Study
Abstract Body: Background: To massively scale up efforts to diagnose and treat hypertension, different screening strategies have been proposed (population-wide screening campaigns and healthcare facility-based “opportunistic” screening). However, no studies have compared their impact on cardiovascular disease (CVD) prevention in low-resource settings.
Objective: To compare hypertension treatment coverage, CVD events, and CVD deaths in Bangladesh from three different screening strategies.
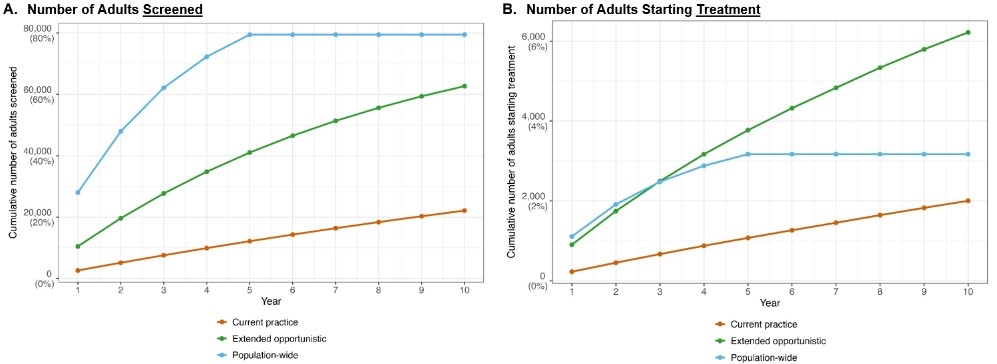
Methods: We developed a discrete-time microsimulation model populated with data from the 2018 Bangladesh WHO STEPS survey. Over 10 years, hypertension diagnosis and treatment, CVD events (strokes and ischemic heart disease), and deaths were estimated for a model population (100,000 adults without hypertension diagnosis or CVD history) under 3 scenarios: (1) current practice of limited opportunistic screening in public healthcare facilities (20% of patients screened); (2) extended opportunistic screening in public healthcare facilities (80% of patients screened); and (3) one-time population-wide screening targeting 80% population coverage over 5 years. In (1) and (2), patients visiting public healthcare facilities (30% of population) could be screened multiple times over the 10 years. Ten-year CVD risk was calculated using WHO CVD prediction models recalibrated with country-specific Global Burden of Disease data.
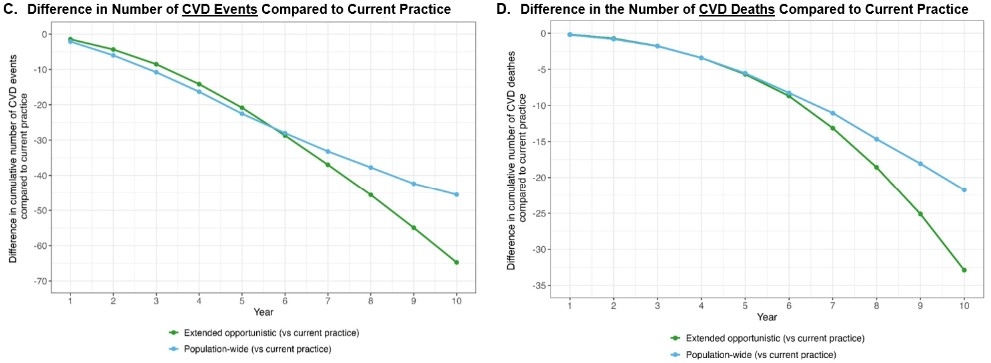
Results: Under current practice, 22,129 adults (out of N=100,000) could be screened over 10 years and 2,002 would start treatment (Figure, Panels A and B); in this scenario, 12,117 CVD events and 1,548 deaths would occur. In the extended opportunistic screening scenario, 62,680 adults would be screened and 6,222 would initiate treatment. With population-wide screening, 79,482 would be screened, and treatment would begin in 3,171 adults. Compared to current practice (Panels C and D), extended opportunistic screening and population-wide screening could prevent 65 and 46 more CVD events, and 33 and 22 CVD deaths per 100,000 over 10 years, respectively. Among adults aged ≥40 years (40% of the total population), the estimated impact on CVD burden was doubled (e.g., 65-70 averted CVD deaths per 100,000).
Conclusion: Despite the intuitive appeal of population-wide screening, the most effective screening strategy to increase screening yield and prevent CVD events in Bangladesh and likely other low-resource settings is extended opportunistic screening in public health care facilities.
Ogungbe, Bunmi
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Hu, Xiao
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Hussain, Tasfia
(
Emory University
, Atlanta , Georgia , United States )
Nguyen, Binh
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Abrar, Ahmad
(
NHF-B
, Dhaka , Bangladesh )
Jubayer, Shamim
(
National Heart Foundation
, Dhaka , Bangladesh )
Choudhury, Sohel
(
National Heart Foundation Hospital
, Dhaka , Bangladesh )
Bhuiyan, Mahfuzur Rahman
(
National Heart Foundation
, Dhaka , Bangladesh )
Moran, Andrew
(
Columbia University Medical Center
, New York , New York , United States )
Commodore-mensah, Yvonne
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Brady, Tammy
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Appel, Lawrence
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Matsushita, Kunihiro
(
JOHNS HOPKINS UNIVERSITY
, Baltimore , Maryland , United States )
Marklund, Matti
(
Johns Hopkins University
, Baltimore , Maryland , United States )