Socioeconomic Disparities in Cardiac Rehabilitation Perceptions and Delivery Mode Preferences: A Nationally Representative Survey Among Diverse Cardiac Patients.
Abstract Body: Background: Cardiac rehabilitation (CR) is essential to secondary cardiovascular disease prevention and management of cardiac patients. Despite its proven benefits, CR remains underutilized with enrollment and completion rates ranging from 10-30% in the US. Yet, there is a scarcity of nationally representative data among diverse populations on socioeconomic differences in barriers and beliefs of CR participation and delivery mode preferences.
Hypothesis: The perceptions (barriers, beliefs), CR delivery mode preferences, and CR utilization (prior enrollment) varies by socioeconomic status (SES) among CR-eligible individuals.
Methods: We conducted an anonymous national electronic survey from March 2023 to January 2024 of individuals self-reporting a prior CR-eligible diagnosis. The 22-item CR Barriers Scale assessed perceived barriers to CR enrollment and participation using a 5-point Likert scale (strongly disagree to strongly agree). A 13-item, validated questionnaire assessed 4 subscales pertaining to patients’ beliefs about CR, each rated on a 5-point Likert scale (strongly disagree to strongly agree): perceived necessity, concerns about exercise, practical barriers and perceived suitability. CR delivery mode preferences were ascertained (eg, virtual, at-home, etc.). Mean barriers and belief scores as well as delivery mode preferences were stratified by SES. Low SES was defined as ≤ high school education, Medicaid insurance, or uninsured. High SES was defined as > high school education and non-Medicaid health insurance. Responses were analyzed using descriptive statistics with R software.
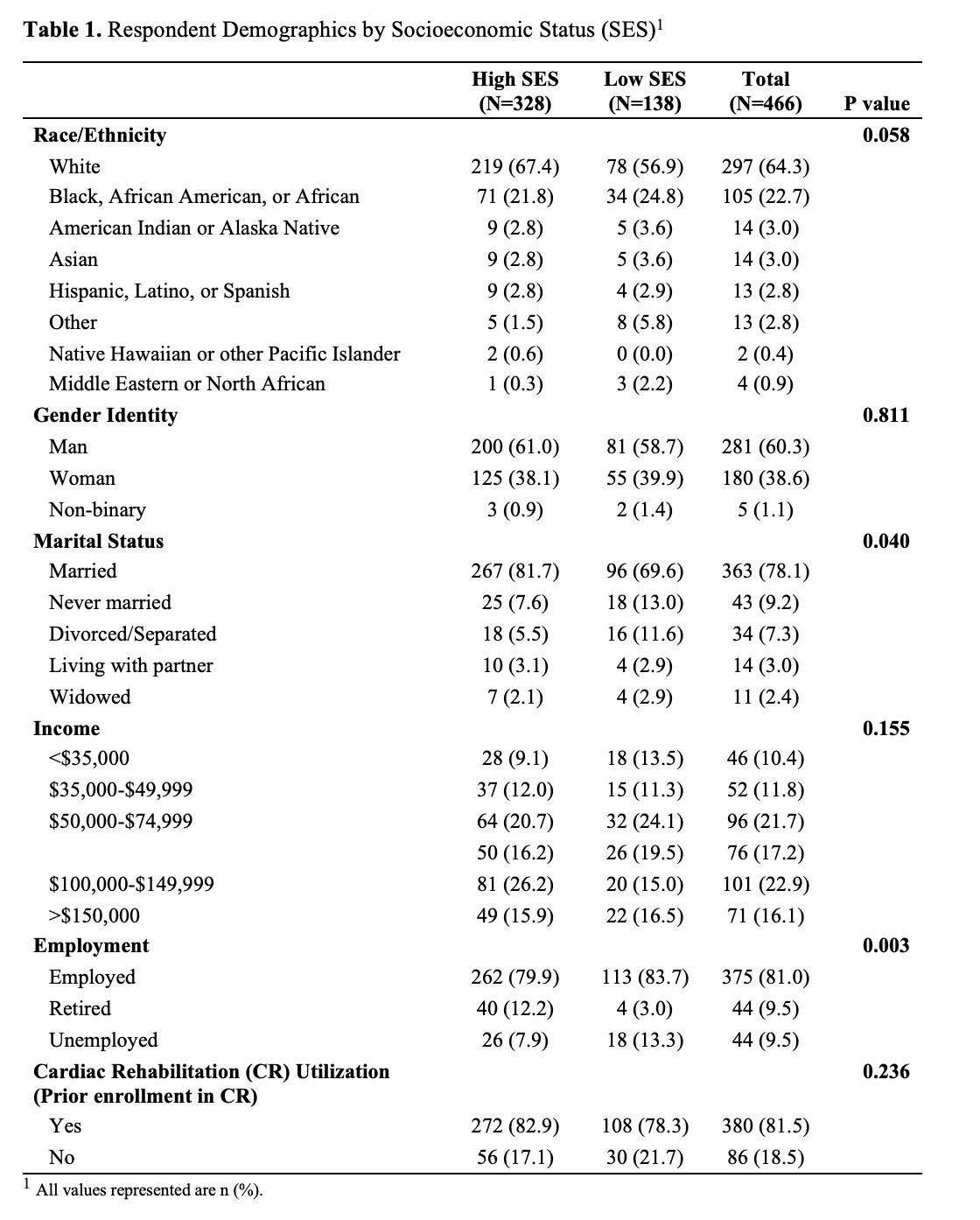
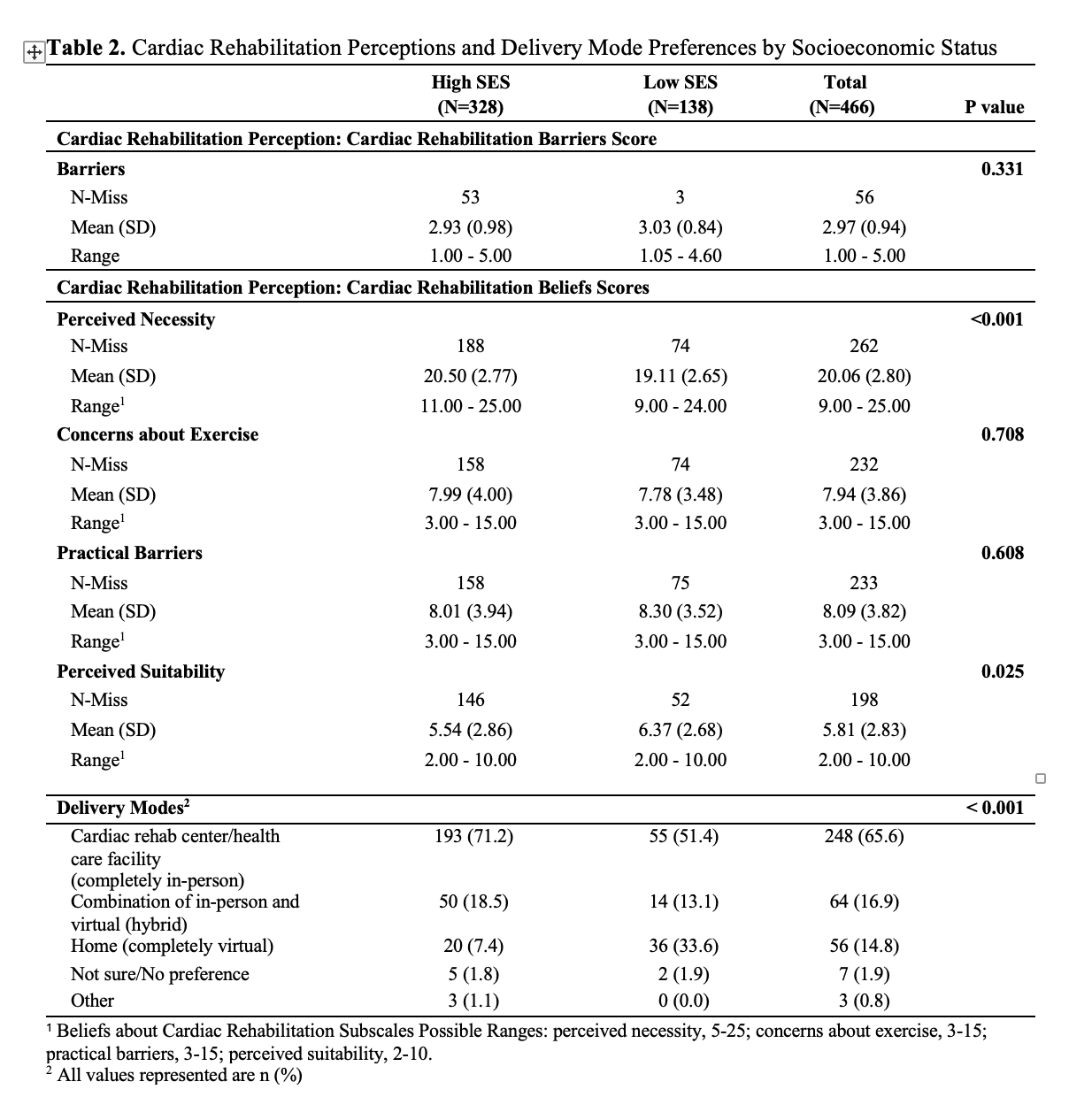
Results: A total of 466 participants completed the survey (38.1% women, 30.6% minoritized racial/ethnic group, 29.6% low SES, 95% response rate) (Table 1). The majority indicated prior enrollment in CR (81.5%) with no difference by SES. CR barrier scores did not differ significantly by SES (p=0.331) (Table 2). Beliefs about CR perceived necessity and perceived suitability differed by SES (p<0.001 and p=0.025), but beliefs regarding concerns about exercise and practical barriers did not. The low SES group reported a higher preference for completely at-home CR compared to the high SES group (33.6% vs 7.4%, p<0.001).
Conclusion: Our findings suggest that CR beliefs varied by SES while utilization did not. For CR-eligible patients experiencing socioeconomic disadvantage, at-home CR may be a preferred alternative to center-based CR to increase CR participation and adherence.
Anyetei-anum, Grace Patrice
(
Mayo Clinic Alix School of Medicine
, Rochester , Minnesota , United States )
Abraham, Helayna
(
Baylor Heart and Vascular Institute
, Dallas , Texas , United States )
Averkamp, Natalie
(
Mayo Clinic
, Rochester , Minnesota , United States )
Johnson, Matthew
(
Mayo Clinic
, Rochester , Minnesota , United States )
Krogman, Ashton
(
, Rochester , Minnesota , United States )
Clark, Donald
(
University of Mississippi
, Jackson , Mississippi , United States )
Echols, Melvin
(
Morehouse School of Medicine
, Atlanta , Georgia , United States )
Hall, Michael And Jo Alice
(
Morehouse School of Medicine
, Atlanta , Georgia , United States )
Hodgman, Karen
(
, Rochester , Minnesota , United States )
Kaihoi, Brian
(
Mayo Clinic
, Rochester , Minnesota , United States )
Kopecky, Stephen
(
, Rochester , Minnesota , United States )
Leth, Shawn
(
, Rochester , Minnesota , United States )
Malik, Shaista
(
University of California
, Irvine , California , United States )
Marsteller, Jill
(
Johns Hopkins Bloomberg School of Public Health
, Baltimore , Maryland , United States )
Mathews, Lena
(
Johns Hopkins
, Baltimore , Maryland , United States )
Scales, Robert
(
Mayo Clinic
, Scottsdale , Arizona , United States )
Shultz, Adam
(
, Rochester , Minnesota , United States )
Taylor, Bryan
(
Mayo Clinic
, Jacksonville , Florida , United States )
Schulte, Phillip
(
Mayo Clinic
, Rochester , Minnesota , United States )
Thomas, Randal
(
, Rochester , Minnesota , United States )
Wong, Nathan
(
University of California
, Irvine , California , United States )
Olson, Thomas
(
, Rochester , Minnesota , United States )
Brewer, Laprincess
(
, Rochester , Minnesota , United States )
Author Disclosures:
Grace Patrice Anyetei-Anum:DO have relevant financial relationships
;
Research Funding (PI or named investigator):American Heart Association Research Supplement to Promote Diversity in Science:Active (exists now)
| Brian Kaihoi:No Answer
| Stephen Kopecky:No Answer
| Shawn Leth:No Answer
| Shaista Malik:No Answer
| Jill Marsteller:No Answer
| Lena Mathews:DO NOT have relevant financial relationships
| Robert Scales:No Answer
| Adam Shultz:DO NOT have relevant financial relationships
| Bryan Taylor:No Answer
| Phillip Schulte:No Answer
| Helayna Abraham:No Answer
| Randal Thomas:No Answer
| Nathan Wong:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Amgen, Novartis, Regeneron, Novo Nordisk:Active (exists now)
; Speaker:Kaneka:Past (completed)
; Speaker:Novartis:Active (exists now)
; Consultant:Novartis, Ionis, HeartLung:Active (exists now)
; Advisor:Amgen:Active (exists now)
| Thomas Olson:No Answer
| LaPrincess Brewer:DO NOT have relevant financial relationships
| Natalie Averkamp:DO have relevant financial relationships
;
Employee:Illumina, Inc :Past (completed)
; Individual Stocks/Stock Options:Vertex:Past (completed)
; Individual Stocks/Stock Options:Pfizer:Past (completed)
; Individual Stocks/Stock Options:Illumina, Inc:Active (exists now)
; Independent Contractor:Medtronic:Past (completed)
| Matthew Johnson:No Answer
| Ashton Krogman:No Answer
| Donald Clark:No Answer
| Melvin Echols:No Answer
| Michael and Jo Alice Hall:DO have relevant financial relationships
;
Consultant:Artivion:Active (exists now)
; Consultant:OrthoQuidel:Active (exists now)
| karen hodgman:No Answer