Infrared Sensor Evaluation for Noninvasive Screening and Early triage in Acute Coronary Syndromes: The iSENSE-ACS Multicenter Study
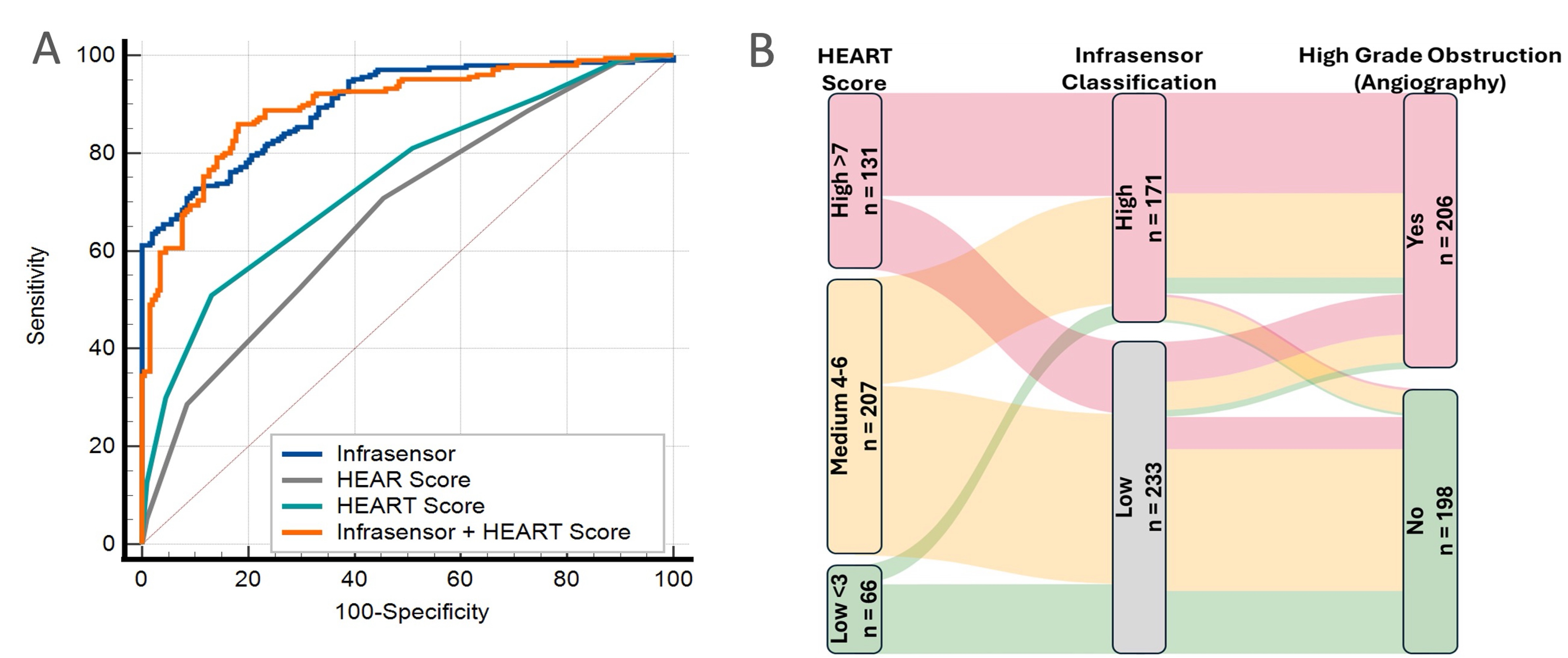
Abstract Body (Do not enter title and authors here): Background: With the rising prevalence of non-ST-elevation acute coronary syndrome (NSTE-ACS) relative to ST-elevation, current guidelines show gaps in the early identification of patients with severe coronary artery disease (CAD) who require time-sensitive reperfusion therapies. This study evaluated the diagnostic utility of a wrist-worn, transdermal infrared spectrophotometric biosensor (Infrasensor) in comparison with standard ECG and blood biomarker-based risk assessment for the early diagnosis and triage of NSTE-ACS and severe obstructive CAD, including cases with total coronary occlusion, referred to as occlusion myocardial infarction (OMI). Methods: In this prospective, multicenter study, 776 subjects were enrolled across 21 sites in two countries and grouped into five analytical cohorts. Evaluations included Infrasensor data, HEART (history, ECG, age, risk factors, and high-sensitivity troponin) and HEAR (without troponin) risk scores, coronary angiography (n = 445), and 30-day clinical follow-up. We implemented machine learning models using a leave-one-cohort-out external validation approach to predict the primary angiographic endpoint of OMI or severe obstructive CAD (defined as>70% stenosis in any coronary artery or >50% stenosis in the left main coronary artery). The secondary model included a final discharge diagnosis of NSTE-ACS, coronary revascularization, or death within 30 days. Results: Severe obstructive CAD was identified in 215 (48%), including 92 (20%) diagnosed as OMI. The primary model showed an area under the ROC curve (AUC) of 0.91 (95% confidence interval, CI: 0.88–0.93), outperforming both HEAR (AUC, 0.64; 95% CI: 0.60-0.68) and HEART (AUC, 0.68;95% CI: 0.64-0.72) risk scores, respectively (P<0.001, Figure 1A). A rule-in strategy using the Infrasensor model demonstrated 90% specificity and 88% positive predictive value, with a 68% net reclassification improvement (95% CI: 54%–82%) over the HEART score (Figure 1B). The secondary model yielded an AUC of 0.92 (95% CI: 0.86–0.94) and achieved 94% sensitivity and 86% negative predictive value for ruling out the composite clinical outcomes. Conclusion: The Infrasensor model significantly outperformed standard guideline-based risk stratification in identifying high-risk CAD and OMI. This wearable, noninvasive technology can safely enhance early triage and decision-making in emergency settings for patients with NSTE-ACS, offering substantial diagnostic improvement over existing methods.
Sengupta, Partho
(
Rutgers RWJ Medical School
, New Brunswick , New Jersey , United States )
Jamthikar, Ankush
(
Rutgers RWJ Medical School
, New Brunswick , New Jersey , United States )
Sandhaus, Marc
(
Rutgers RWJ Medical School
, New Brunswick , New Jersey , United States )
Yanamala, Naveena
(
Rutgers RWJ Medical School
, New Brunswick , New Jersey , United States )
Maganti, Kameswari
(
Rutgers University
, New Brunswick , New Jersey , United States )
Titus, Jitto
(
RCE Technologies
, Acworth , Georgia , United States )
Bhavnani, Sanjeev
(
Scripps Translational Science Insti
, La Jolla , California , United States )
Daniels, Lori
(
UC San Diego
, Del Mar , California , United States )
Peacock, William
(
BAYLOR COLLEGE MEDICINE
, Houston , Texas , United States )
Sengupta, Shantanu
(
Sengupta Hospital and Research Institute
, Nagpur , Maharashtra State , India )
Author Disclosures:
Partho Sengupta:DO have relevant financial relationships
;
Advisor:RCE Technologies:Active (exists now)
; Advisor:HeartSciences:Active (exists now)
| Shantanu Sengupta:DO NOT have relevant financial relationships
| Ankush Jamthikar:No Answer
| Marc Sandhaus:No Answer
| Naveena Yanamala:No Answer
| Kameswari Maganti:DO NOT have relevant financial relationships
| Jitto Titus:No Answer
| Sanjeev Bhavnani:No Answer
| Lori Daniels:DO have relevant financial relationships
;
Advisor:Curemetrix:Past (completed)
; Other (please indicate in the box next to the company name):Tosoh - Clinical Outcomes Adjudication Committee:Past (completed)
; Advisor:Abbott:Past (completed)
; Advisor:Siemens:Past (completed)
; Consultant:Roche:Active (exists now)
; Consultant:QuidelOrtho:Past (completed)
| William Peacock:DO have relevant financial relationships
;
Consultant:Abbott:Past (completed)
; Ownership Interest:Emergencies in Medicine:Active (exists now)
; Ownership Interest:Comprehensive Research Associates:Active (exists now)
; Consultant:Werfen:Active (exists now)
; Ownership Interest:Aseptiscope:Active (exists now)
; Consultant:Roche:Active (exists now)
; Consultant:RCE:Active (exists now)
; Consultant:Radiometer:Active (exists now)
; Consultant:Quidel:Active (exists now)
; Consultant:Osler:Active (exists now)
; Consultant:Oragenics:Active (exists now)
; Consultant:Cerebraai:Active (exists now)
; Consultant:Bristol Meyer Squibb:Active (exists now)
; Consultant:Brainbox:Active (exists now)
; Consultant:Biocogniv:Active (exists now)