Outpacing Tradition: Conduction System Pacing Demonstrates Superior Outcomes to Biventricular Pacing for HFrEF.
Abstract Body (Do not enter title and authors here): Background Cardiac resynchronization therapy (CRT) improves outcomes in heart failure patients with reduced ejection fraction (HFrEF) and ventricular dyssynchrony. While biventricular pacing (BVP) is the standard approach, it produces non-physiologic activation and leaves up to one-third of patients as non-responders. Conduction system pacing (CSP)—including His bundle and left bundle branch pacing—offers a more physiologic alternative by engaging native conduction pathways.We conducted a meta-analysis of randomized controlled trials (RCTs) comparing CSP and BVP to assess differences in clinical and echocardiographic outcomes
Methods: A systematic search of PubMed, Scopus, and Cochrane databases identified 8 RCTs including 477 patients with HFrEF undergoing CRT. Outcomes analyzed included QRS duration, NYHA functional class, left ventricular ejection fraction (LVEF), end-systolic volume (LVESV), pacing threshold, and procedural time. Fixed-effect meta-analyses were performed, and heterogeneity was assessed using the I2 statistic.
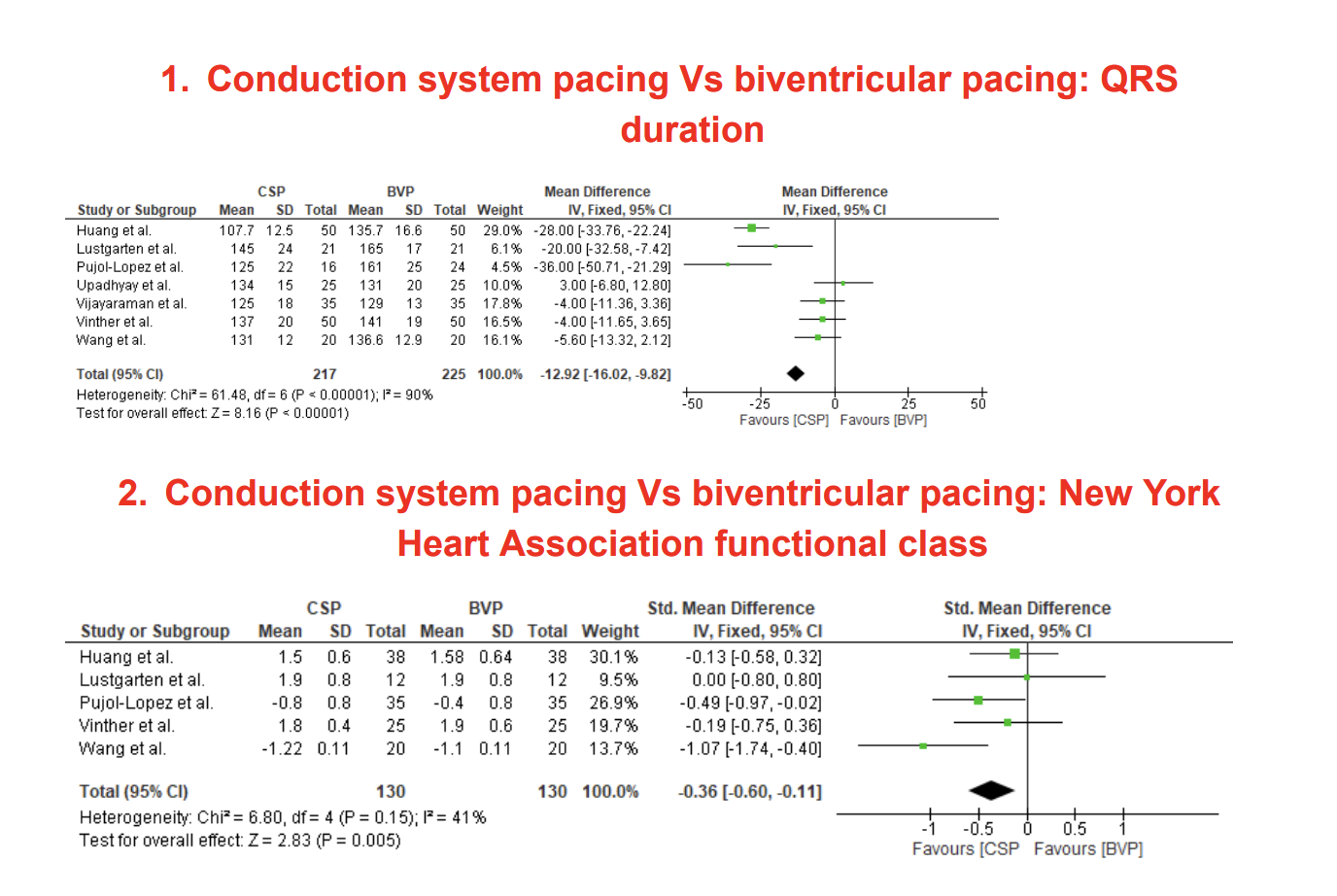
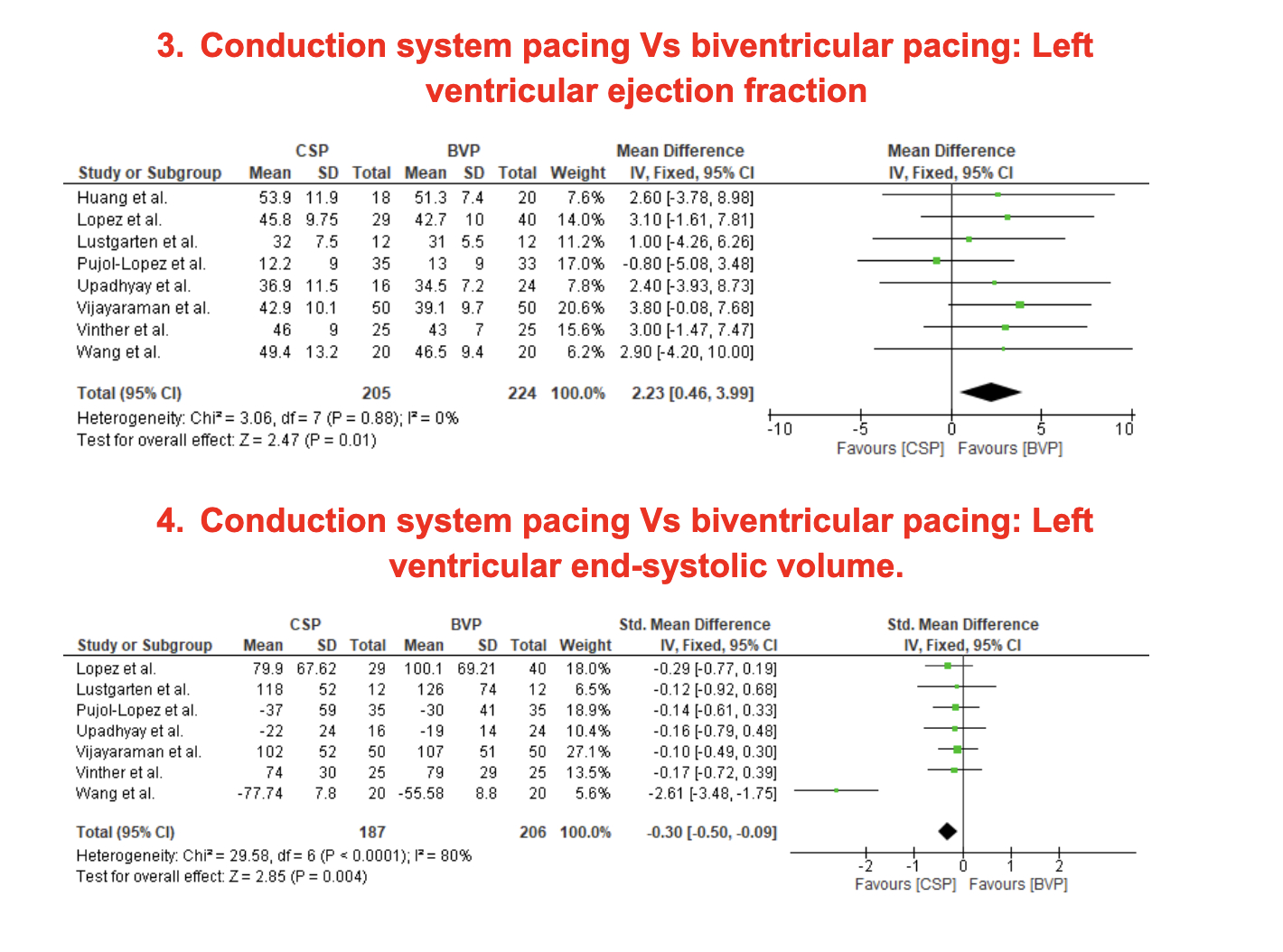
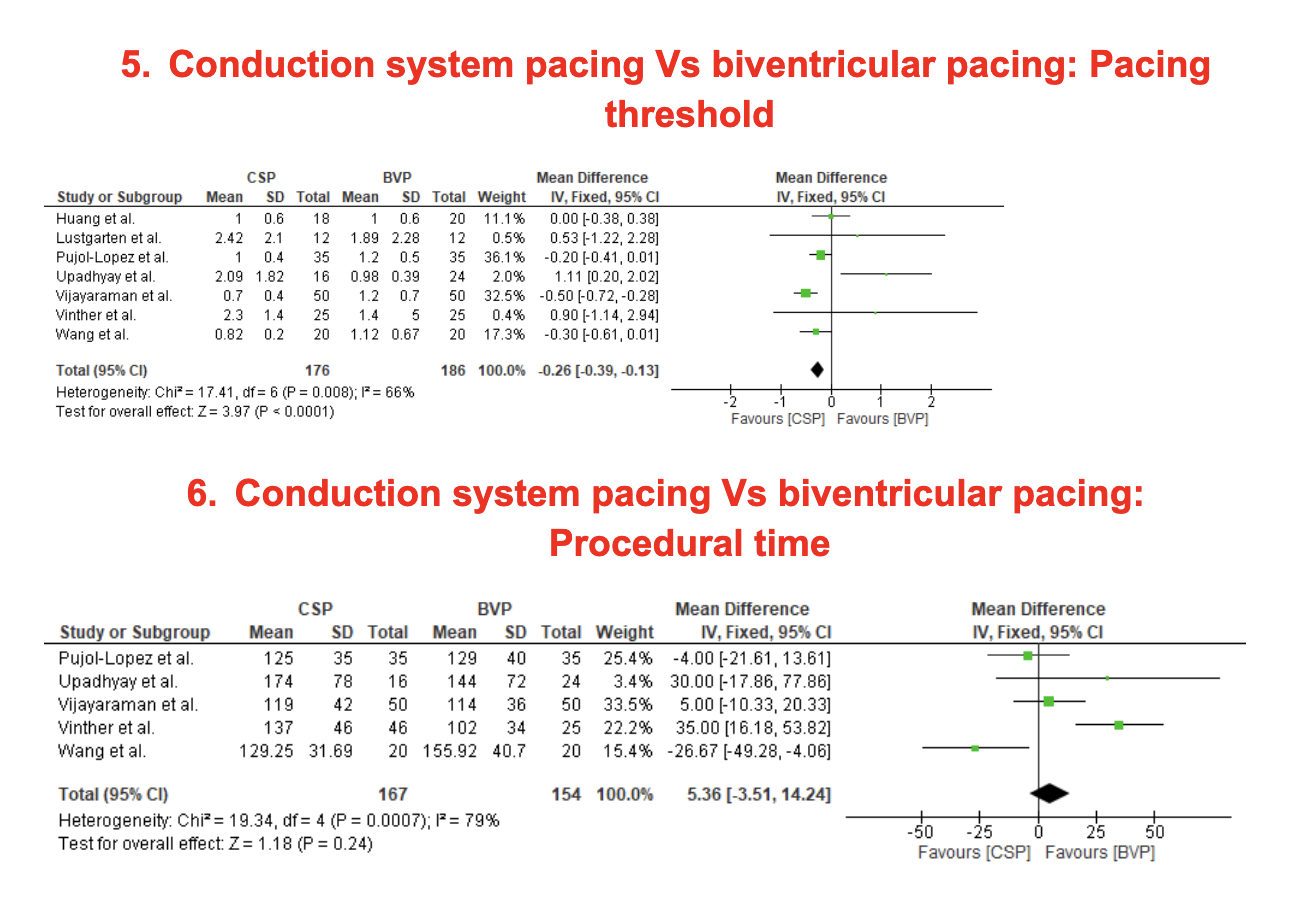
Results: Compared to BVP, CSP significantly improved key resynchronization metrics:
-QRS Duration: CSP shortened QRS more than BVP (MD: -12.92 ms, 95% CI: -16.02 to -9.82, P < 0.00001). -NYHA Class: Functional status was superior with CSP (SMD: -0.36, 95% CI: -0.60 to -0.11, P = 0.005). -LVEF: Greater improvement in LVEF with CSP (MD: +2.23%, 95% CI: 0.46 to 3.99, P = 0.01). -LVESV: CSP led to more favorable reverse remodeling (SMD: -0.30, 95% CI: -0.50 to -0.09, P = 0.004). -Pacing Threshold: Lower pacing threshold observed with CSP (MD: -0.26 V, 95% CI: -0.39 to -0.13, P < 0.0001). -Procedural Time: No significant difference (MD: +5.36 min, 95% CI: -3.51 to 14.24, P = 0.24).
Conclusion This meta-analysis of randomized trials shows CSP offers superior electrical and clinical outcomes compared to BVP in CRT-eligible HFrEF patients. CSP led to greater QRS narrowing, improved NYHA class, enhanced ejection fraction, and reduced end-systolic volume. Pacing thresholds were lower with CSP, supporting device longevity. Although procedural time was higher, the clinical benefits may outweigh this limitation. These findings support CSP as a promising first-line CRT strategy, warranting broader adoption and further long-term evaluation.
Sharma, Arundhati
(
Guthrie/Robert Packer Hospital
, Sayre , Pennsylvania , United States )
Sharma, Anubhuti
(
Guthrie/Robert Packer Hospital
, Sayre , Pennsylvania , United States )
Daid, Simranpreet Singh
(
Roger William Medical center
, Providence , Rhode Island , United States )
Sharma, Saurabh
(
Guthrie/Robert Packer Hospital
, Sayre , Pennsylvania , United States )
Author Disclosures:
Arundhati Sharma:DO NOT have relevant financial relationships
| Anubhuti Sharma:DO NOT have relevant financial relationships
| Simranpreet Singh Daid:DO NOT have relevant financial relationships
| Saurabh Sharma:DO NOT have relevant financial relationships