Prognosis of Cardiovascular-Kidney-Metabolic (CKM) Stages: The Dallas Heart Study
Abstract Body (Do not enter title and authors here): Background: The recent AHA presidential advisory on Cardiovascular-Kidney-Metabolic Syndrome (CKM) proposed a novel staging scheme, but limited data exist regarding the associations of CKM Stages with incident cardiovascular events and mortality.
Methods: We included participants in the Dallas Heart Study, a population-sampled cohort from Dallas County, who attended study Visit 1 (2000-2002) and underwent protocol measurement of body composition, lipids, fasting blood sugar, serum creatinine, NT-proBNP, hs-cTnT, urinary albumin and creatinine, coronary artery calcium by cardiac CT (CAC), and cardiac function and mass by cardiac MRI. CKM Stages were defined as per AHA CKM definitions: Stage 0 – no CKM risk factors; 1 – excess or dysfunctional adiposity; 2 – metabolic risk factors and/or chronic kidney disease; 3 – subclinical cardiovascular diseases [CAC, left ventricular hypertrophy or dysfunction by cardiac MRI, elevated cardiac biomarkers (NT-proBNP or hs-cTnT), high AHA-PREVENT or KDIGO scores]; 4 – prevalent cardiovascular diseases [coronary heart disease (CHD), heart failure (HF), atrial fibrillation, stroke]. Participants were followed for fatal and non-fatal clinical outcomes, including CHD, HF, and stroke through December 31th 2018. Multivariable Cox proportional hazard models were used to assess the relationship of the CKM Stage with incident events compared to absent CKM or Stage 1, adjusting for age, sex, and race.
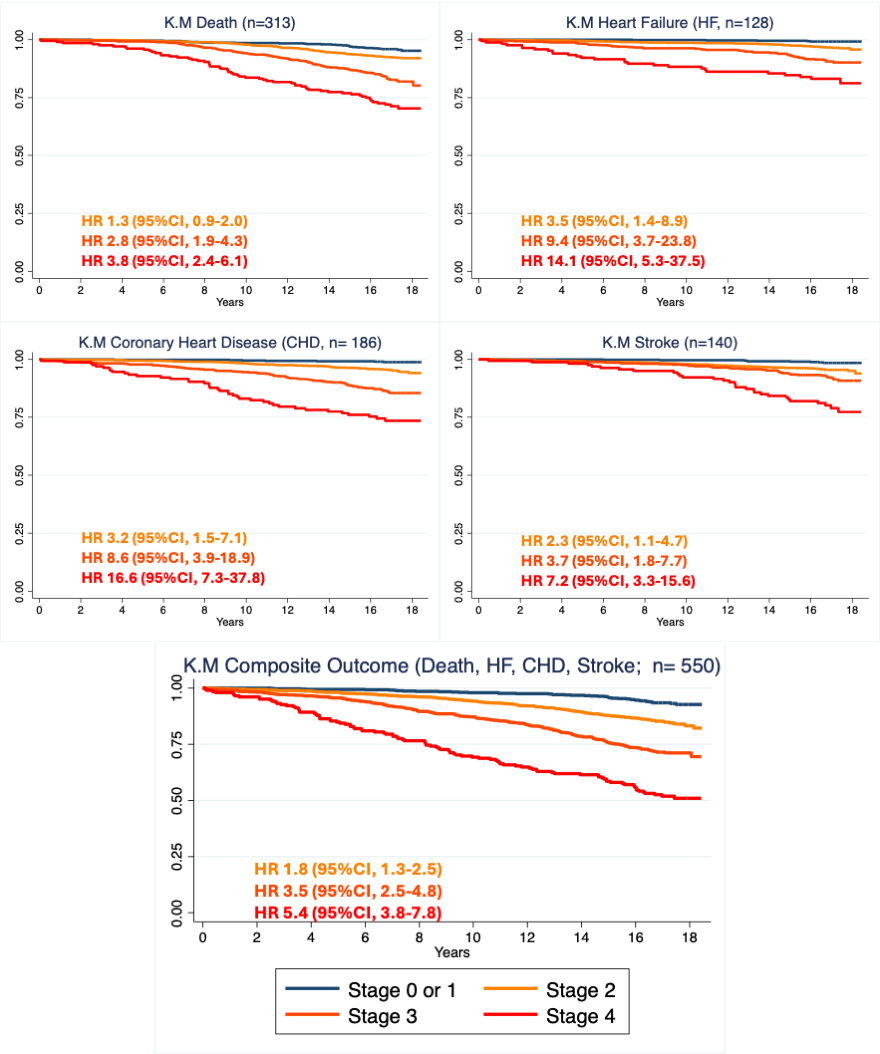
Results: Among the 2,991 participants (age 44±10 years, 56% female, 50% reported non-Hispanic Black race), CKM stage prevalence was 9% Stage 0, 14% Stage 1, 47% Stage 2, 22% Stage 3, and 7% Stage 4. Over a median follow-up of 16.9 (IQR 16.4 -17.6) years, 19% died or developed CHD, HF, or stroke. No significant differences in risk were observed between Stage 0 and Stage 1 for composite and individual outcomes. Compared to those with Stage 0 or 1 CKM, a graded association was observed between greater CKM Stage 2-4 and heightened risk of composite CHD, HF, stroke, or death [HR 1.8 (95% CI 1.3-2.5), 3.5 (2.5-4.8), 5.4 (3.8-7.8), respectively] in adjusted model. Similar trends were observed for each component of the composite (Figure).
Conclusion: Over 17 years of follow-up, individuals with CKM Stage 1 did not experience worse outcomes than those free of CKM Stage. CKM Stages 2, 3, and 4 were associated with a stepwise higher risk of all cause mortality and incident CHD, HF, and stroke compared to those with Stage 0 or 1 CKM.
Shelbaya, Khaled
(
UT Southwestern Medical Center
, Dallas , Texas , United States )
Yang, Yimin
(
UT Southwestern Medical Center
, Dallas , Texas , United States )
Lamberson, Victoria
(
UT Southwestern Medical Center
, Dallas , Texas , United States )
Zeleke, Yinun
(
UT Southwestern Medical Center
, Dallas , Texas , United States )
Joshi, Parag
(
UT Southwestern Medical Center
, Dallas , Texas , United States )
Rohatgi, Anand
(
UT SOUTHWESTERN
, Dallas , Texas , United States )
Ayers, Colby
(
UT Southwestern Medical Center
, Dallas , Texas , United States )
Khera, Amit
(
UT Southwestern
, Dallas , Texas , United States )
De Lemos, James
(
UT SOUTHWESTERN MEDICAL CTR
, Dallas , Texas , United States )
Neeland, Ian
(
University Hospitals - Case Western
, Cleveland , Ohio , United States )
Ndumele, Chiadi
(
JOHNS HOPKINS HOSPITAL
, Silver Spring , Maryland , United States )
Shah, Amil
(
UT Southwestern Medical Center
, Dallas , Texas , United States )
Author Disclosures:
Khaled Shelbaya:DO have relevant financial relationships
;
Employee:Alexion Pharmaceuticals Inc:Active (exists now)
| Ian Neeland:DO have relevant financial relationships
;
Consultant:Boehringer Ingelheim:Past (completed)
; Advisor:MJH Life Sciences:Active (exists now)
; Advisor:Novo Nordisk:Past (completed)
; Speaker:Bayer:Active (exists now)
; Speaker:Eli Lilly:Active (exists now)
; Consultant:Eli Lilly:Past (completed)
; Speaker:Boehringer Ingelheim:Active (exists now)
| Chiadi Ndumele:DO NOT have relevant financial relationships
| Amil Shah:DO NOT have relevant financial relationships
| Yimin Yang:DO NOT have relevant financial relationships
| Victoria Lamberson:DO NOT have relevant financial relationships
| Yinun Zeleke:No Answer
| Parag Joshi:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Novartis:Active (exists now)
; Consultant:New Amsterdam Pharma:Past (completed)
; Consultant:Kaneka:Past (completed)
; Consultant:Novartis:Past (completed)
; Research Funding (PI or named investigator):Kaneka:Past (completed)
; Research Funding (PI or named investigator):Eli Lilly:Active (exists now)
| Anand Rohatgi:DO have relevant financial relationships
;
Consultant:Raydel:Past (completed)
; Consultant:JP Morgan:Past (completed)
; Consultant:Johnson and Johnson:Past (completed)
; Other (please indicate in the box next to the company name):LabCorp:Active (exists now)
; Other (please indicate in the box next to the company name):Quest:Active (exists now)
; Research Funding (PI or named investigator):CSL Behring:Past (completed)
| Colby Ayers:DO have relevant financial relationships
;
Consultant:NIH:Active (exists now)
| Amit Khera:DO NOT have relevant financial relationships
| James de Lemos:DO have relevant financial relationships
;
Independent Contractor:Amgen, Inc.:Active (exists now)
; Independent Contractor:Verve:Active (exists now)
; Consultant:Siemen's:Past (completed)
; Independent Contractor:Jannsen:Active (exists now)
; Independent Contractor:Astra Zeneca:Past (completed)
; Independent Contractor:Merck:Active (exists now)
; Independent Contractor:Eli Lilli:Active (exists now)
; Independent Contractor:Varian:Active (exists now)
; Independent Contractor:Regerenon Pharmaceuticals:Active (exists now)