Partial Anomalous Pulmonary Venous Return: An Uncommon Cause of Refractory Hypoxemia Following Coronary Artery Bypass Grafting
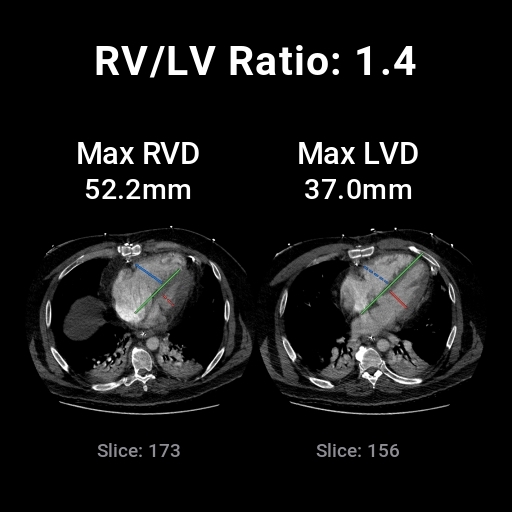
Abstract Body (Do not enter title and authors here): Background: Severe hypoxemia after coronary artery bypass grafting (CABG) is a critical complication. Common preoperative risk factors include chronic pulmonary disease, myocardial infarction, and diabetes. Potential postoperative causes of hypoxemia include atelectasis, pleural effusion, and pulmonary edema. Rarely, anatomical abnormalities such as partial anomalous pulmonary venous return (PAPVR) may also contribute. Case Presentation: A 47-year-old male with gastroesophageal reflux disease and obesity presented with left-sided chest pain. He was diagnosed with non-ST elevation myocardial infarction (NSTEMI) and hypertensive urgency. Cardiac catheterization revealed multivessel coronary artery disease, and he underwent CABG. Intraoperative transesophageal echocardiography (TEE) showed normal biventricular function without intracardiac shunting. Postoperatively, the patient developed persistent hypoxemia requiring high ventilatory support. He became hypotensive, unresponsive to medical therapy and intra-aortic balloon pump (IABP), necessitating venovenous extracorporeal membrane oxygenation (VV ECMO) initiation. Transthoracic echocardiography (TTE) revealed moderate right ventricular (RV) enlargement with preserved left ventricular function. Following clinical improvement, he was decannulated, but hypoxemia recurred within 24 hours, and ECMO was restarted. A contrast-enhanced CT revealed RV enlargement and PAPVR, characterized by left upper lobe vertical vein draining into the left brachiocephalic vein, as shown in the images. Repeat TEE confirmed the diagnosis. Treatment with milrinone, inhaled nitric oxide, and inhaled epoprostenol led to significant hemodynamic and oxygenation improvement. Given the diagnosis and clinical course, the patient was referred for surgical correction of the PAPVR. Discussion: PAPVR is a rare congenital abnormality where one or more pulmonary veins drain into the systemic circulation rather than the left atrium, creating a left-to-right shunt. While often asymptomatic, it can become clinically significant when right ventricle strain occurs, such as post-CABG stress. Conclusion: PAPVR, though rare, should be a part of differential diagnosis in persistent hypoxemia and right ventricular dysfunction after CABG. Early recognition through multimodal imaging, including CT and TEE, is critical. ECMO may be necessary for stabilization while pursuing definitive surgical management.
Azhar, Masood
(
Baptist Health South Florida
, Miami , Florida , United States )
Chaparro, Sandra
(
Baptist Health South Florida
, Miami , Florida , United States )
Fernandez, Javier
(
University of Miami
, Miami , Florida , United States )
Jimenez, Javier
(
Baptist Health South Florida
, Miami , Florida , United States )
Author Disclosures:
Masood Azhar:DO NOT have relevant financial relationships
| Sandra Chaparro:No Answer
| Javier Fernandez:DO NOT have relevant financial relationships
| Javier Jimenez:No Answer