Comparative Outcomes of Multi-Arterial versus Single Arterial Grafting in Patients with Reduced Left Ventricular Ejection Fraction Undergoing Coronary Artery Bypass Grafting: A Systematic Review and Meta-Analysis
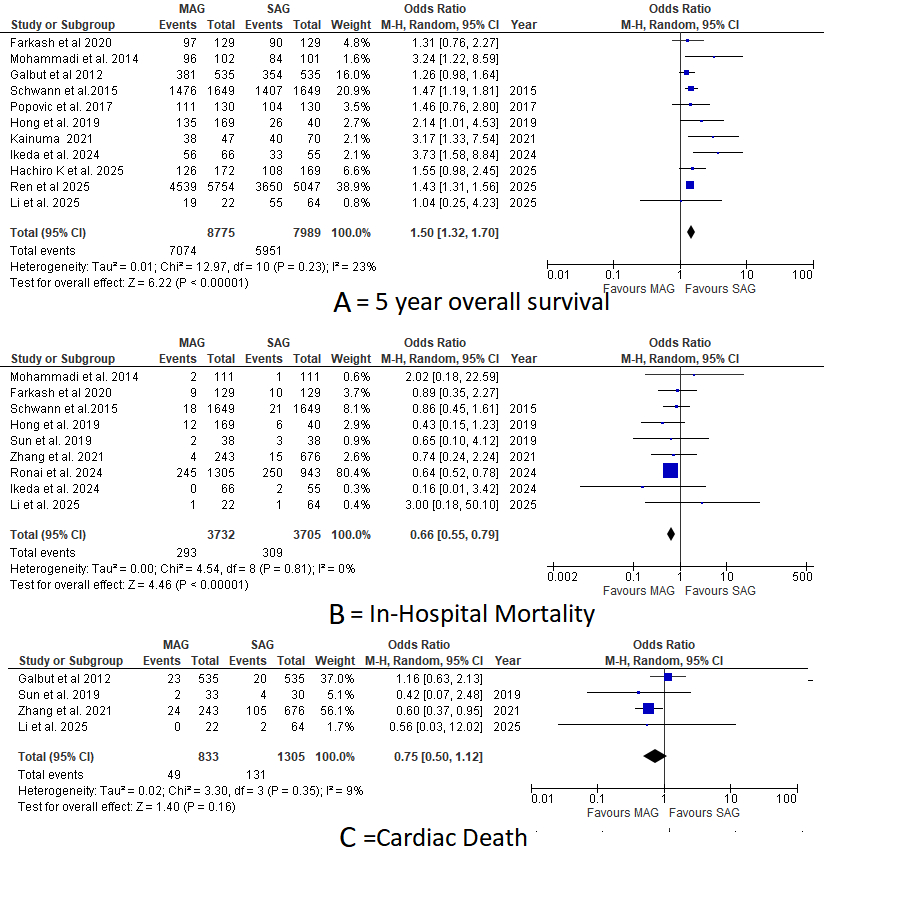
Abstract Body (Do not enter title and authors here): Background Patients with ischemic heart failure and reduced ejection fraction (HFrEF) remain at high risk despite surgical revascularization. While single arterial grafting (SAG) is standard in CABG, multi-arterial grafting (MAG) may offer better outcomes. However, its benefits in patients with reduced ejection fraction remain unclear. Aims To evaluate whether MAG offers superior survival and clinical outcomes compared to SAG in patients with reduced LVEF undergoing CABG. Methods A systematic search of PubMed, Embase, and Cochrane Central was conducted for studies comparing MAG and SAG in patients with LVEF <50%. Primary outcomes included 5-year overall survival, cardiac death, and in-hospital mortality. Secondary outcomes were MACE, perioperative MI, atrial fibrillation, reoperation, repeat revascularization, IABP use, stroke, and postoperative complications. Results A total of 19,976 patients were included (MAG: 10,306; SAG: 9,670). MAG was associated with significantly higher 5-year survival (OR: 1.50; 95% CI: 1.32–1.70; p < 0.00001) and lower in-hospital mortality (OR: 0.66; 95% CI: 0.55–0.79; p < 0.00001), with a trend toward reduced cardiac death (OR: 0.75; 95% CI: 0.50–1.12; p = 0.16). No significant differences were seen in MACE (OR: 0.72; 95% CI: 0.49–1.04; p = 0.08), MI (OR: 0.72; 95% CI: 0.48–1.06; p = 0.09), or repeat revascularization (OR: 0.62; 95% CI: 0.23–1.68; p = 0.35). Reoperation was marginally lower with MAG (OR: 0.56; 95% CI: 0.31–1.00; p = 0.05). There were no significant differences in stroke (OR: 1.23; 95% CI: 0.92–1.65; p = 0.16), atrial fibrillation (OR: 0.93; 95% CI: 0.55–1.56; p = 0.78), IABP use (OR: 0.75; 95% CI: 0.49–1.15; p = 0.18), hospital stay (MD: 0.03; 95% CI: –0.64 to 0.70; p = 0.93), ICU stay (MD: 0.17; 95% CI: –0.30 to 0.63; p = 0.48), dialysis (OR: 0.92; 95% CI: 0.61–1.38; p = 0.68), or sternal wound infection (OR: 1.56; 95% CI: 0.83–2.94; p = 0.17). Conclusions In patients with reduced LVEF undergoing CABG, MAG is associated with improved 5-year survival and lower in-hospital mortality without increased perioperative complications. These findings support broader consideration of MAG in this high-risk group.
Henna, Fathimathul
(
Dubai medical college for girls
, Dubai , United Arab Emirates )
Shahid, Iqra
(
kemu
, Lahore , Pakistan )
Author Disclosures:
Zaryab Bacha:DO NOT have relevant financial relationships
| Fathimathul Henna:DO NOT have relevant financial relationships
| Iqra Shahid:DO NOT have relevant financial relationships
| Mian Zahid Jan Kakakhel:DO NOT have relevant financial relationships
| Javeria Javed:No Answer
| Ali Fida Khan:DO NOT have relevant financial relationships
| Muhammad Abdullah Ali:DO NOT have relevant financial relationships
| Muhammad Osama:DO NOT have relevant financial relationships
| Umama Alam:DO NOT have relevant financial relationships
| Abdullah Afridi:No Answer
| Maheen Sheraz:No Answer