Clinical and Demographic Predictors of Rapid Aortic Stenosis Progression: Moving Toward Individualized Surveillance Strategies
Abstract Body (Do not enter title and authors here): Introduction Aortic stenosis (AS) is the most common valvular heart disease requiring intervention in the US. Untreated symptomatic AS carries a one-year mortality rate of up to 50%, while timely diagnosis allows for effective treatment. AS progresses gradually over years and is typically monitored with surveillance echocardiography. AS progression rates vary significantly between individuals. Current guidelines recommend uniform surveillance intervals, which may result in unnecessary imaging for slow progressors and delayed diagnosis for rapid progressors. This study aims to analyze a large echocardiographic dataset with longitudinal follow-up to identify risk factors for rapid AS progression, ultimately supporting individualized surveillance strategies based on patient-specific risk profiles.
Methods This retrospective study included patients with serial echocardiograms between 2011 and 2021. A natural language processing algorithm was developed to extract AS severity from each report. Rapid AS progression was defined as an increase in Vmax of ≥0.3 m/s per year, and severe AS was defined as Vmax ≥4.0 m/s. Multivariable logistic regression models were constructed to evaluate clinical factors associated with rapid progression.
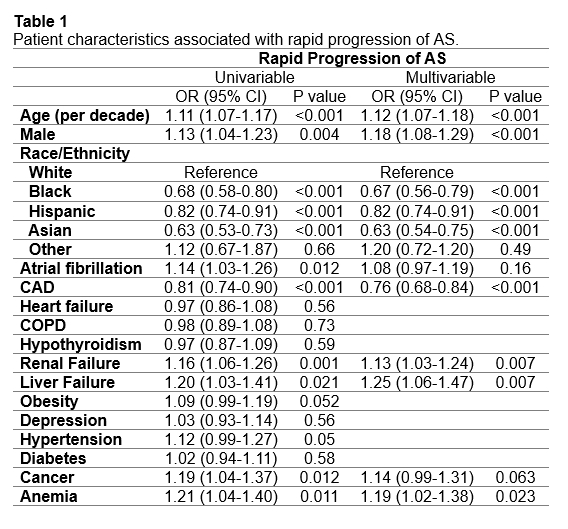
Results The study included 24,821 patients with borderline, mild, or moderate AS. Mean follow-up was 4.1 years. 2,492 patients experienced rapid AS progression and 1,998 progressed to severe AS. Factors associated with rapid progression included older age (OR 1.12, 95% CI 1.07–1.18), male sex (OR 1.18, 95% CI 1.08–1.29), renal disease (OR 1.13, 95% CI 1.03–1.24), liver disease (OR 1.25, 95% CI 1.06–1.47), and anemia (OR 1.19, 95% CI 1.02–1.38) while coronary artery disease was associated with a lower risk (OR 0.76, 95% CI 0.68–0.84). Among racial and ethnic groups, white patients had the highest risk of rapid AS progression.
Conclusion Approximately 10% of patients studied experienced rapid disease progression. Older age, male sex, white race, and clinical factors such as renal disease, liver disease, and anemia were associated with rapid AS progression. These patients may benefit from closer follow-up and shorter echocardiographic surveillance intervals. This work lays the foundation for developing a personalized risk score to inform patient-specific surveillance intervals based on individual risk profiles.
Ho, Michael
(
Kaiser Permanente
, Los Angeles , California , United States )
Wu, Yi-lin
(
Kaiser Permanente
, Pasadena , California , United States )
Xie, Fagen
(
Kaiser Permanente
, Los Angeles , California , United States )
Chen, Wansu
(
Kaiser Permanente
, Los Angeles , California , United States )
Lee, Mingsum
(
Kaiser Permanente
, Los Angeles , California , United States )
Author Disclosures:
Michael Ho:DO NOT have relevant financial relationships
| Yi-Lin Wu:No Answer
| Fagen Xie:No Answer
| Wansu Chen:No Answer
| Mingsum Lee:DO NOT have relevant financial relationships
Au Michael, Shah Nilay, Reynolds Kristi, An Jaejin, Zhang Yiyi, Zhou Mengnan, Choi Soonie, Zhou Hui, Harrison Teresa, Mefford Matthew, Lee Mingsum, Yang Eugene
4367966_File000000.jpg
You have to be authorized to contact abstract author. Please, Login