Cost Effectiveness of Intravascular Use for Lower Extremity Deep Venous Procedures in Real World Practice
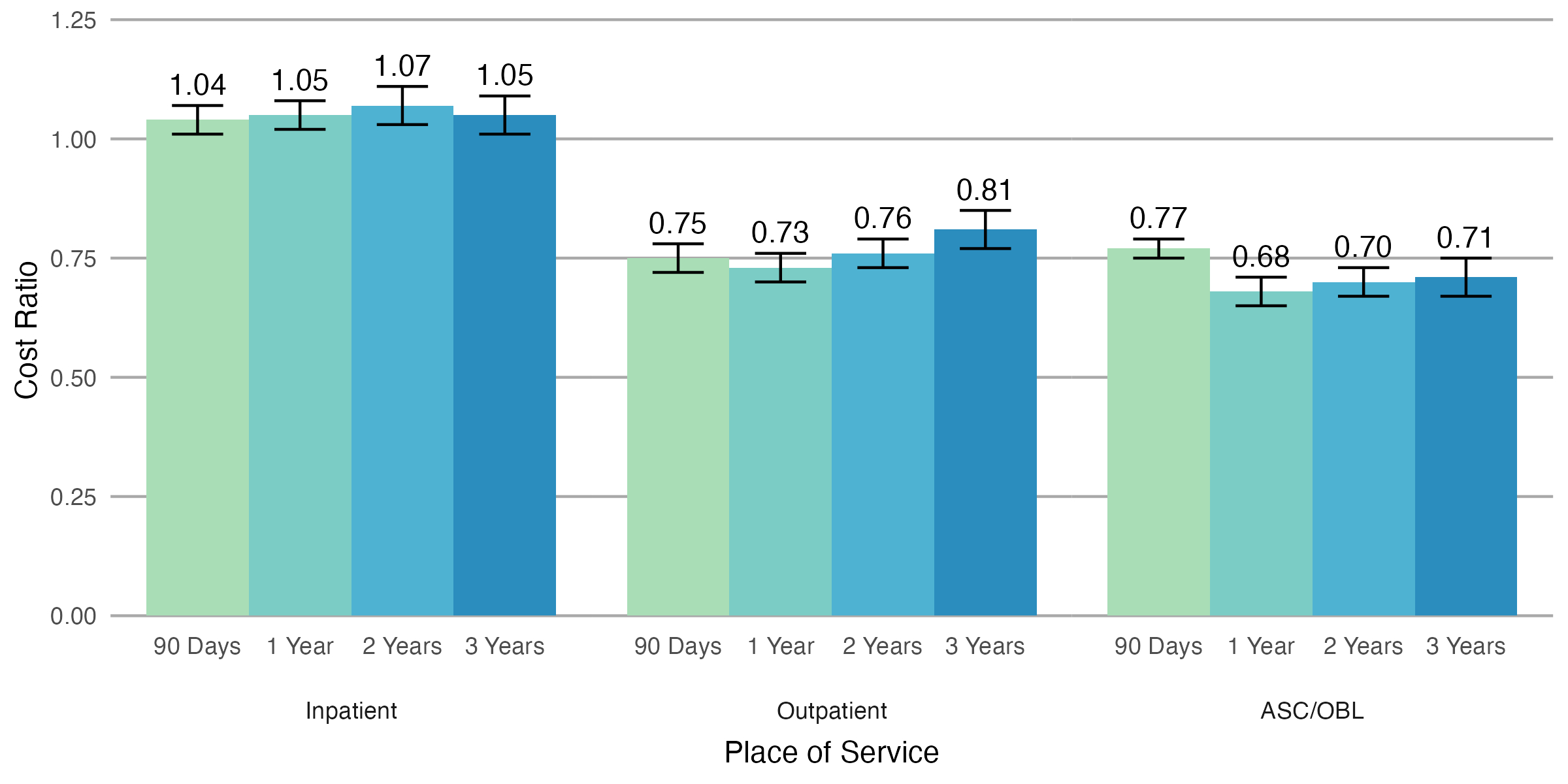
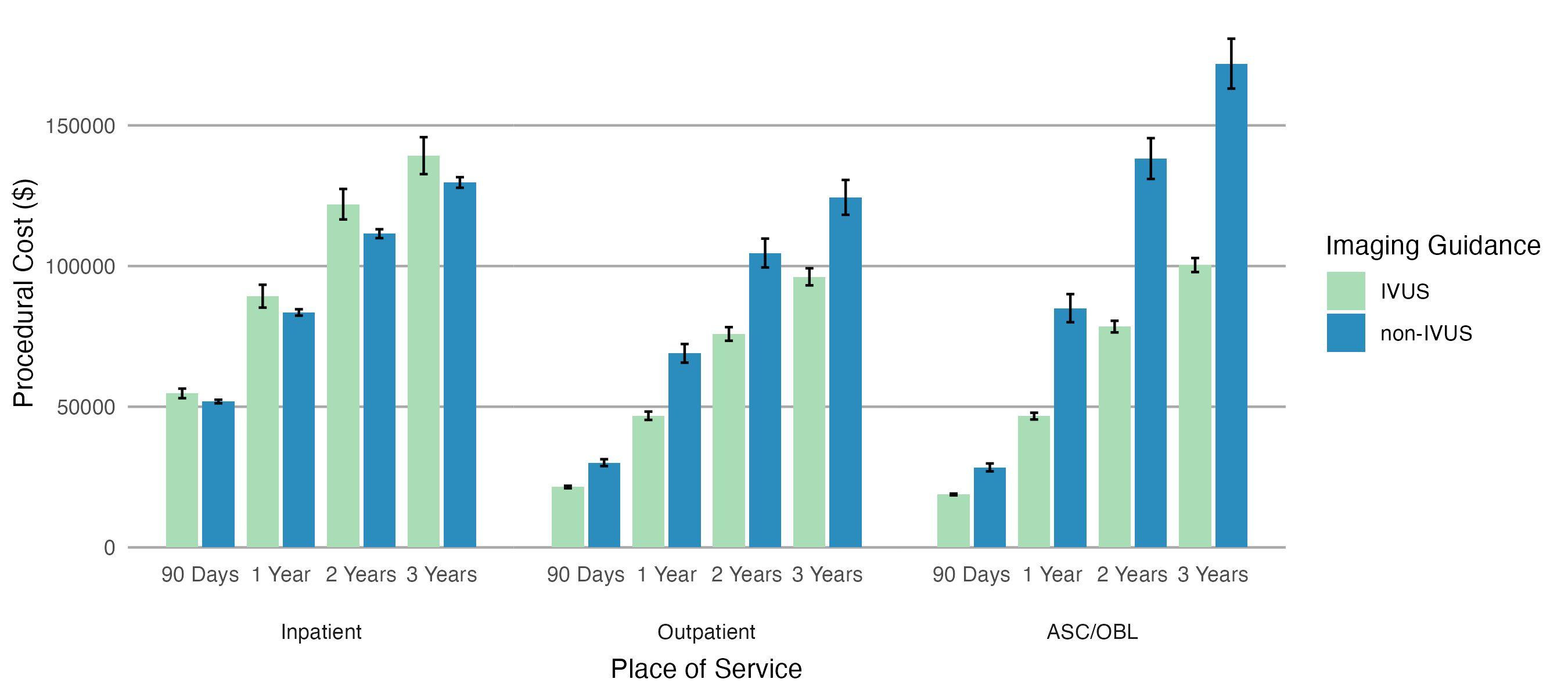
Abstract Body (Do not enter title and authors here): Introduction The use of intravascular ultrasound (IVUS) to guide lower extremity deep venous stent placement is associated with improved identification of the degree of maximal vessel stenosis, vessel obstruction, and thrombus burden, compared to venography alone. As the US medical system moves towards value-based care, the financial impact of interventional tools requires close consideration. Currently, there are limited evaluations of the cost effectiveness of IVUS during venous procedures. Research Question This study seeks to examine the cost-effectiveness of IVUS in lower extremity deep venous interventions. Methods Medicare fee-for-service claims data from 2016 through 2021 for beneficiaries aged ≥ 65 years undergoing lower extremity venous interventions with stent placement, thrombolysis, and/or thrombectomy were analyzed. Cost ratios between IVUS-guided and non-IVUS-guided procedures were assessed using gamma regression, adjusting for demographic and clinical variables. Results A total of 52,610 patients were included, with 42.6% undergoing IVUS-guided procedures. IVUS utilization varied by setting, with higher usage in hospital-based outpatient centers (75.3%) and ambulatory surgical centers/outpatient-based laboratories (ASC/OBL; 86.4%) compared to inpatient hospitalizations (10.4%). Among inpatient procedures, IVUS-guided venous intervention was associated with greater cost than non-IVUS procedures at 90 days, with an adjusted cost ratio of 1.04 (95% CI 1.01-1.07), yet was associated with an average 0.6-day shorter hospitalization (p < 0.001; Figure 1, Figure 2). There were marginal increased costs associated with use of IVUS in inpatient procedures persisting through one- and three-years follow-up, with adjusted cost ratios of 1.05 (95% CI 1.02-1.08) and 1.05 (95% CI 1.02-1.09), respectively. In contrast, IVUS use was associated with significant cost savings in outpatient settings, with adjusted cost ratios of 0.71 (95% CI 0.69-0.73) in hospital-based outpatient settings and 0.75 (95% CI 0.73-0.78) in ASC/OBL at 90 days. These cost savings persisted at one- and three-year follow-up. Conclusions IVUS-guided venous intervention was associated with cost savings in outpatient and ASC/OBL settings, while maintaining near cost equivalence in inpatient settings. These findings suggest that in addition to the clinical benefit of IVUS for venous intervention, IVUS is a cost-effective strategy, particularly in the outpatient setting.
Herzig, Matthew
(
Beth Israel Deaconess Medical Cente
, Boston , Massachusetts , United States )
Kim, Joseph
(
Beth Israel Deaconess Medical Cente
, Boston , Massachusetts , United States )
Desai, Kush
(
Northwestern University
, Chicago , Illinois , United States )
Sabri, Saher
(
MedStar Health
, Washington , District of Columbia , United States )
Patel, Parag
(
Mayo Clinic
, Rochester , Minnesota , United States )
Li, Siling
(
Beth Israel Deaconess Medical Cente
, Boston , Massachusetts , United States )
Song, Yang
(
Beth Israel Deaconess Medical Cente
, Boston , Massachusetts , United States )
Secemsky, Eric
(
Beth Israel Deaconess Medical Cente
, Boston , Massachusetts , United States )
Author Disclosures:
Matthew Herzig:DO NOT have relevant financial relationships
| Joseph Kim:DO NOT have relevant financial relationships
| Kush Desai:DO have relevant financial relationships
;
Consultant:BD:Past (completed)
; Consultant:Terumo:Active (exists now)
; Consultant:Cook Medical:Active (exists now)
; Consultant:Medtronic:Active (exists now)
; Consultant:Philips:Past (completed)
; Consultant:Penumbra:Active (exists now)
; Consultant:WL Gore:Active (exists now)
; Consultant:Boston Scientific:Active (exists now)
| Saher Sabri:No Answer
| Parag Patel:DO NOT have relevant financial relationships
| Siling Li:No Answer
| Yang Song:DO NOT have relevant financial relationships
| Eric Secemsky:No Answer