Explainable Machine Learning for Risk Stratification of Major Adverse Cardiac Events Using Clinical and Imaging Data
Abstract Body (Do not enter title and authors here): Background Accurate prediction of major adverse cardiac events (MACE) is critical for guiding cardiovascular care. Traditional risk scores such as the Pooled Cohort Equations (PCE) and PREVENT rely solely on clinical variables and may underutilize valuable imaging data. With increasing availability of coronary artery calcium (CAC) CT scans, there is a growing opportunity to leverage multimodal data and interpretable machine learning (ML) models for enhanced risk stratification.
Research Questions Can an interpretable ML model incorporating clinical, medication, ECG, and CAC CT-derived features outperform traditional clinical risk scores (PCE, PREVENT) in predicting MACE? Which features contribute most outcome prediction?
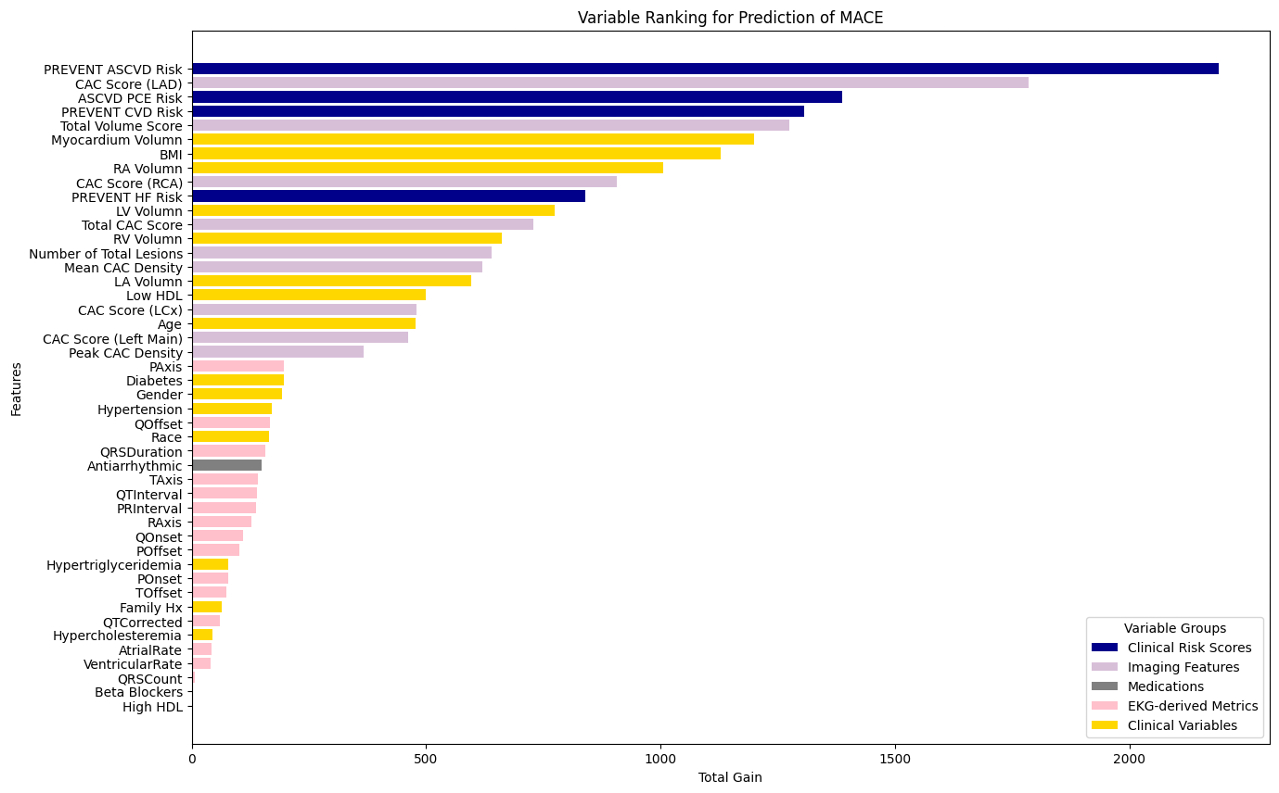
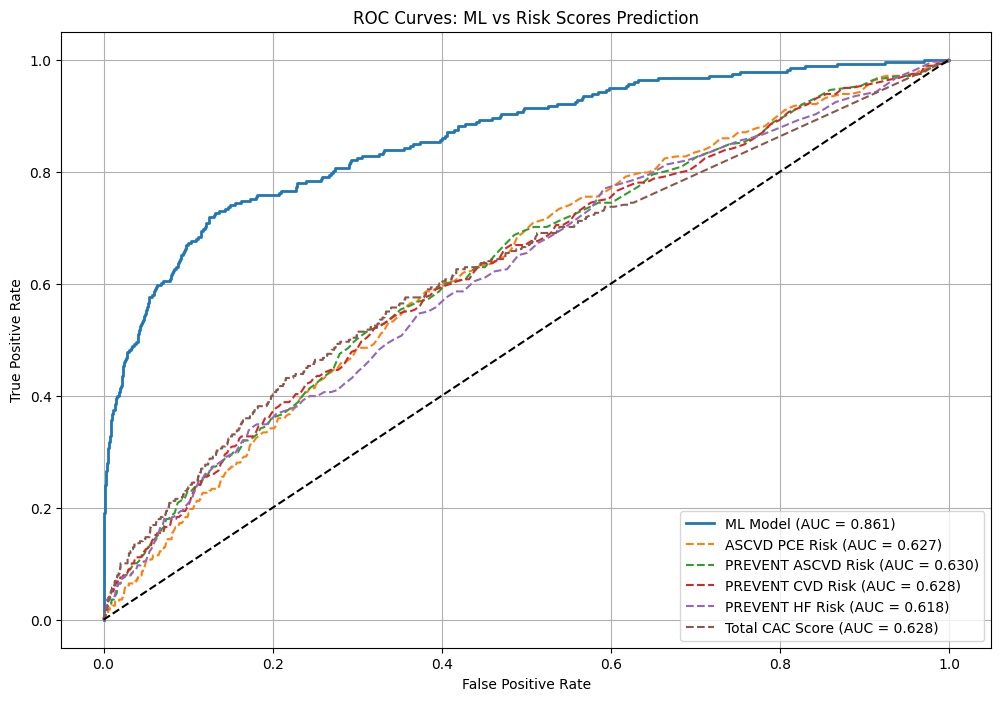
Methods In this retrospective cohort study, 7,828 asymptomatic individuals without known cardiovascular disease underwent CAC CT between 2010–2023 for risk stratification. A total of 52 features were used for model development, including 16 clinical variables, 7 medication variables, 15 ECG-derived parameters, and 14 CT-derived imaging features (including Agatston score, CAC volume and density, and cardiac chamber volumes). An XGBoost model was trained using stratified 10-fold cross-validation with hyperparameter optimization via grid search. Model performance was evaluated by area under the receiver operating characteristic curve (AUROC) and compared against the Pooled Cohort Equations (PCE), PREVENT score, and total CAC score. Feature importance was assessed using total gain.
Results/Data The mean age was 57.9 years; 44.6% were women and 11.5% were Black. The overall MACE rate was 4.6%. Non-zero CAC was observed in 56.6% of participants, with a median CAC score of 44.2 (IQR 5.3, 145) among those with calcifications. The ML model achieved an AUROC of 0.861 for MACE prediction, outperforming the PCE (AUROC = 0.627), PREVENT (AUROC = 0.630), and total CAC score alone (AUROC = 0.628). The most informative predictors included the PREVENT and PCE risk scores, CAC in the left anterior descending artery, total CAC volume, myocardial and right atrial volumes, and regional CAC scores.
Conclusion An interpretable ML model incorporating clinical and imaging features significantly outperformed traditional risk scores in predicting MACE. Key imaging and clinical variables were identified as principal contributors to risk, demonstrating the potential of interpretable ML to augment cardiovascular risk stratification.
Gershon, Gabrielle
(
Emory University
, Atlanta , Georgia , United States )
Yan, Xinyue
(
Emory University
, Atlanta , Georgia , United States )
Adibi, Ali
(
Georgia Tech
, Atlanta , Georgia , United States )
Gabriel, Roy
(
Georgia Tech
, Atlanta , Georgia , United States )
Kittisut, Nattakorn
(
Georgia Tech
, Atlanta , Georgia , United States )
Rapaka, Saikiran
(
Siemens
, Newark , New Jersey , United States )
De Cecco, Carlo
(
Emory University
, Atlanta , Georgia , United States )
Van Assen, Marly
(
Emory University
, Atlanta , Georgia , United States )
Author Disclosures:
Gabrielle Gershon:DO NOT have relevant financial relationships
| Xinyue Yan:DO NOT have relevant financial relationships
| Ali Adibi:No Answer
| Roy Gabriel:DO NOT have relevant financial relationships
| Nattakorn Kittisut:DO NOT have relevant financial relationships
| Saikiran Rapaka:DO have relevant financial relationships
;
Employee:Siemens Healthineers:Active (exists now)
; Individual Stocks/Stock Options:Siemens Healthineers:Active (exists now)
| Carlo De Cecco:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Siemens:Active (exists now)
; Research Funding (PI or named investigator):Cleerly:Active (exists now)
| Marly van Assen:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Siemens:Active (exists now)
; Research Funding (PI or named investigator):Cleerly Inc:Active (exists now)