Impact of Obesity on Atrial Mechanical and Electrical Function in Patients Undergoing HFpEF Evaluation – A Propensity-Matched Analysis
Abstract Body (Do not enter title and authors here): Introduction: Obesity is a known risk factor for atrial fibrillation and heart failure with preserved ejection fraction (HFpEF). However, the specific mechanisms through which it affects atrial myopathy remain poorly defined.
Research Question: Is obesity associated with worse anatomical, mechanical, and electrical parameters of atrial function?
Methods: We conducted a retrospective study of patients evaluated for suspected HFpEF at a tertiary care outpatient clinic. Participants were stratified into three groups according to body mass index (BMI): (1) without obesity (BMI < 30 kg/m2), (2) class I obesity (BMI 30–35 kg/m2), and (3) class II or greater obesity (BMI > 35 kg/m2). Propensity score matching was performed for age, sex, hypertension, atrial fibrillation, diabetes mellitus, and chronic kidney disease. Atrial function was assessed by echocardiography, including indexed left atrial volume (LAVI) and left atrial strain during the reservoir (LAS-r), conduit (LAS-cd), and contraction (LAS-ct) phases. Electrical function was evaluated using P wave amplitude and duration on resting 12-lead electrocardiograms. A p-value < 0.05 was considered statistically significant, and 95% confidence intervals were reported.
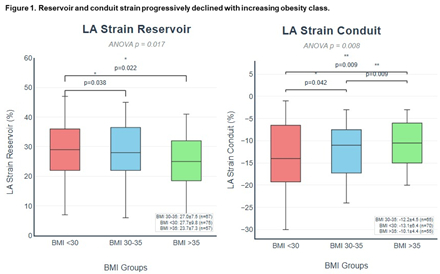
Results: After propensity score matching, 216 patients were included: 81 (37.5%) without obesity, 72 (33.3%) with class I obesity, and 63 (29.2%) with class II or greater obesity. The mean ages were 61.4, 62.0, and 61.7 years, respectively; 70.3% were women. The prevalence of hypertension ranged from 79.4% to 81.9%, and diabetes mellitus from 32.1% to 46.8% across groups. Echocardiographic evaluation revealed a significant and progressive reduction in reservoir and conduit strain values across increasing obesity categories (LAS-r: 27.72 ± 9.82 vs. 27.03 ± 7.51 vs. 23.67 ± 7.27; p = 0.017 and LAS-cd: –13.07 ± 6.38 vs. –12.17 ± 4.52 vs. –10.13 ± 4.45; p = 0.008; Figure 1). No significant differences were observed in contraction strain (p = 0.20), LAVI (p = 0.20), P wave amplitude (p = 0.74), or P wave duration (p = 0.60). As expected, NT-proBNP levels were significantly lower in individuals with higher BMI (636.21 ± 1548.98 vs. 240.71 ± 549.40 vs. 168.33 ± 195.01; p = 0.01).
Conclusion: In this propensity-matched cohort, obesity was associated with progressive impairment in reservoir and conduit atrial strain. No differences were observed in atrial contraction strain, left atrial volume, or electrocardiographic P wave parameters.
Guida, Camila
(
Instituto Dante Pazzanese de Cardio
, Sao Paulo , Brazil )
Farias, Eduardo
(
Instituto Dante Pazzanese de Cardio
, Sao Paulo , Brazil )
Delamain, Tacianne
(
Instituto Dante Pazzanese de Cardio
, Sao Paulo , Brazil )
Shinzato, Mariane
(
Instituto Dante Pazzanese de Cardio
, Sao Paulo , Brazil )
Freitas, Rafaela Andrade Penalva
(
Instituto Dante Pazzanese de Cardio
, Sao Paulo , Brazil )
Franchini, Kleber
(
Instituto Dante Pazzanese de Cardio
, Sao Paulo , Brazil )
Author Disclosures:
Camila Guida:DO NOT have relevant financial relationships
| Eduardo Farias:DO NOT have relevant financial relationships
| Tacianne Delamain:No Answer
| Mariane Shinzato:DO NOT have relevant financial relationships
| RAFAELA ANDRADE PENALVA FREITAS:DO NOT have relevant financial relationships
| Kleber Franchini:DO NOT have relevant financial relationships