The Heart in the Crossfire: Nationwide Insights on Cardiovascular Complications of Cytokine Release Syndrome
Abstract Body (Do not enter title and authors here): Cytokine release syndrome (CRS) is a systemic inflammatory response marked by the excessive release of pro-inflammatory cytokines, commonly triggered by immunotherapies such as CAR T-cell therapy. Cardiovascular complications are an underrecognized but significant aspect of patient outcomes. CRS can lead to hemodynamic instability, cardiac dysfunction, arrhythmias, and endothelial injury, necessitating prompt recognition and management.
A retrospective analysis was performed using the National Inpatient Sample (NIS) to assess the association between CRS and cardiovascular complications. Adult hospitalizations with CRS were identified using ICD-10 code D89.83, with a non-CRS control group. Multivariable logistic regression models adjusted for demographics and comorbidities, including hypertension, diabetes, CKD, obesity, smoking, COVID-19, sepsis, autoimmune diseases (SLE, RA), autologous HSCT, and CAR-T therapy in DLBCL. Results were reported as adjusted odds ratios (aOR) with 95% confidence intervals (CI), and chi-square tests were used for categorical comparisons (p < 0.05 considered significant).
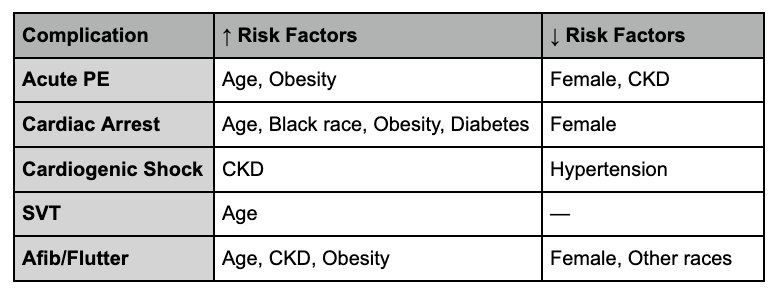
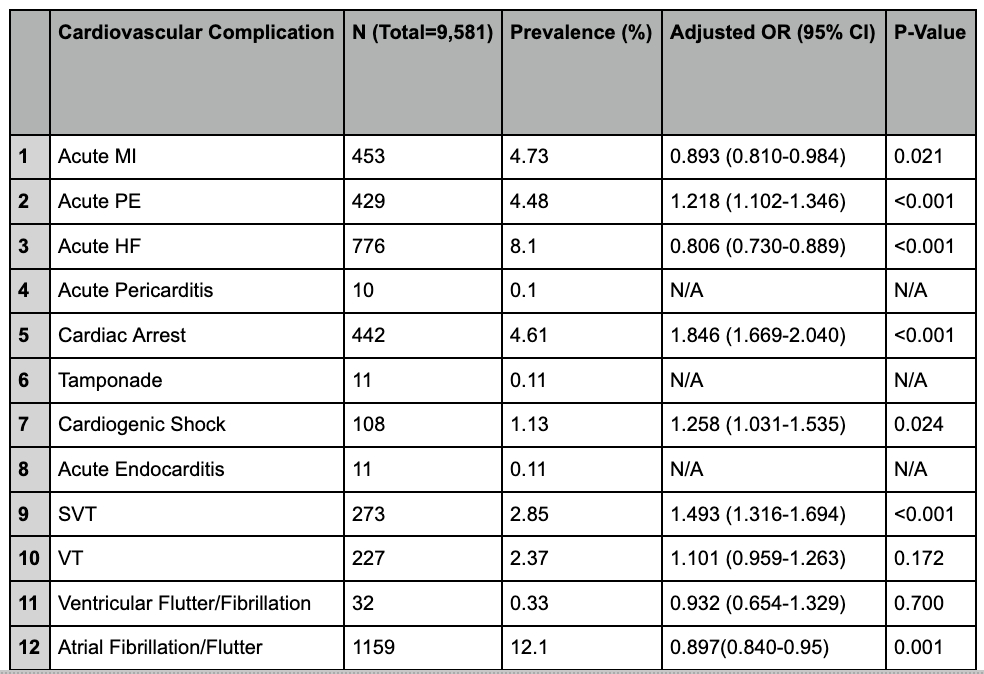
Among 11,261,491 hospitalizations, 9,399 had a diagnosis of CRS. COVID-19 was the most common cause (7,190 cases; 24.96%). After adjustment, CRS was associated with increased risk of acute pulmonary embolism (aOR: 1.218, 95% CI: 1.102–1.346, p < 0.001), cardiac arrest (aOR: 1.846, 95% CI: 1.669–2.040, p < 0.001), cardiogenic shock (aOR: 1.258, 95% CI: 1.031–1.535, p = 0.024), and supraventricular tachycardia (aOR: 1.493, 95% CI: 1.316–1.694, p < 0.001). CRS was associated with decreased risk of acute myocardial infarction (aOR: 0.893, 95% CI: 0.810–0.984, p = 0.021) and heart failure (aOR: 0.806, 95% CI: 0.730–0.889, p < 0.001). No significant association was found with ventricular tachycardia (p = 0.172). Subgroup analysis showed acute PE was associated with older age and obesity, while female sex and CKD were protective. Cardiac arrest was more likely in older, Black, obese, and diabetic patients; female sex was protective. Cardiogenic shock was linked to CKD, while hypertension was paradoxically protective. Atrial fibrillation/flutter was more common in older patients and those with CKD or obesity.
CRS is associated with a heightened risk of several cardiovascular events, particularly PE, cardiac arrest, and SVT. These findings underscore the importance of cardiovascular risk assessment and monitoring in patients with CRS.
Dayal, Manik
(
Rutgers New Jersey Medical School
, Monroe Township , New Jersey , United States )
Shah, Anand
(
Rutgers New Jersey Medical School
, Monroe Township , New Jersey , United States )
Patel, Sagar
(
Rutgers New Jersey Medical School
, Monroe Township , New Jersey , United States )
Afshar, Maryam
(
Rutgers New Jersey Medical School
, Monroe Township , New Jersey , United States )
Author Disclosures:
Manik Dayal:DO NOT have relevant financial relationships
| Anand Shah:No Answer
| Sagar Patel:DO NOT have relevant financial relationships
| MARYAM AFSHAR:No Answer