Nonlinear Association Between Post-Cardiac Arrest Mean Arterial Pressure and Outcome Suggests 85–100 mmHg as the Optimal Range
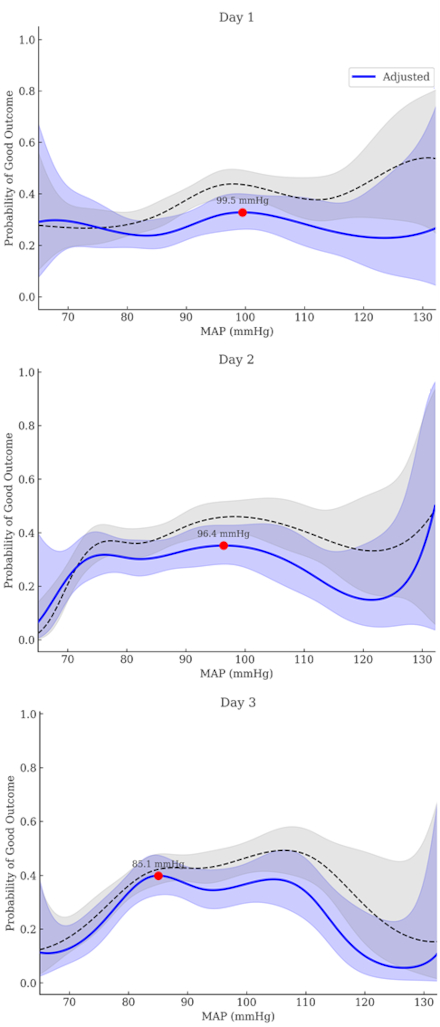
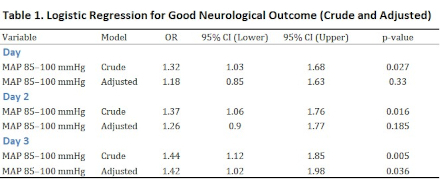
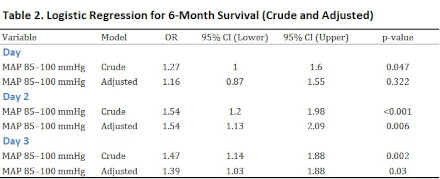
Abstract Body (Do not enter title and authors here): Introduction Post-cardiac arrest care seeks to optimize cerebral perfusion for neurological recovery. Mean arterial pressure (MAP) is a key target in hemodynamic management, but guidelines recommend only a minimal threshold of 60–65 mmHg based on low-certainty evidence. Observational studies report better outcomes with higher MAP, but cannot prove causality. In contrast, randomized controlled trials (RCTs) that adjust MAP show inconsistent results. This discrepancy may reflect confounding in observational data, where higher MAP often indicates lower illness severity, and harm from excessive MAP in some RCT patients. Both study types dichotomized MAP, assuming a linear relationship. However, because both hypotension and hypertension may worsen outcomes, a nonlinear association is plausible. Identifying an optimal MAP range instead of using cutoffs may improve outcomes. Aims We aimed to identify an optimal MAP range associated with the highest probability of neurological recovery, assuming a nonlinear relationship between MAP and outcome. Methods We analyzed data from 1,146 out-of-hospital cardiac arrest survivors in the Korean Hypothermia Network prospective registry. MAPs were calculated for Day 1 (0–24h), Day 2 (30–48h), Day 3 (54–72h), and after return of spontaneous circulation. Restricted cubic spline (RCS) logistic regression modeled nonlinear associations between MAP and good neurological outcome (modified Rankin Scale 0–2 at 6 months). Optimal MAP ranges were derived from spline curves. Logistic regression evaluated associations between maintaining MAP within this range and outcomes, including 6-month survival. Results RCS analysis showed a nonlinear association between MAP and neurological outcome across all time intervals. The MAP values associated with the highest predicted probability of good outcome were 99.5 mmHg on Day 1, 96.4 mmHg on Day 2, and 85.1 mmHg on Day 3. Based on these, the optimal MAP range was defined as 85–100 mmHg. Maintaining MAP within this range was significantly associated with good neurological outcome on Day 3 (adjusted OR 1.42, p = 0.036) and improved survival on Day 2 (adjusted OR 1.54, p = 0.006) and Day 3 (adjusted OR 1.39, p = 0.030). Conclusion MAP and neurological outcome after cardiac arrest appear nonlinearly related. Maintaining MAP between 85 and 100 mmHg was associated with improved neurological recovery and survival, particularly on Days 2 and 3. This range warrants further investigation in interventional trials.
Oh, Joo Suk
(
The Catholic University of Korea, Uijeongbu St. Mary's Hospital
, Uijeongbu-si , Korea (the Republic of) )
Kim, Kiwook
(
The Catholic University of Korea, Uijeongbu St. Mary's Hospital
, Uijeongbu-si , Korea (the Republic of) )
Lee, Byungkook
(
Chonnam National University Hospital
, Gwangju , Korea (the Republic of) )
Lee, Dong Hoon
(
Chung-Ang University Hospital
, Gwangmyeong-si , Korea (the Republic of) )
You, Yeon Ho
(
Chungnam National University Hospital
, Daejeon , Korea (the Republic of) )
Choi, Seung Pill
(
The Catholic University of Korea, Eunpyeong St. Mary's Hospital
, Seoul , Korea (the Republic of) )
Park, Yoo Seok
(
Yonsei University College of Medicine
, Seoul , Korea (the Republic of) )
Author Disclosures:
Joo Suk Oh:DO NOT have relevant financial relationships
| Kiwook Kim:DO NOT have relevant financial relationships
| Byungkook Lee:DO NOT have relevant financial relationships
| Dong Hoon Lee:DO NOT have relevant financial relationships
| Yeon Ho You:No Answer
| Seung Pill Choi:No Answer
| Yoo Seok Park:DO NOT have relevant financial relationships