Concerning Differences in Major Amputation Trends by Hospital Medicaid Proportion, Patient Income and Race/Ethnicity
Abstract Body (Do not enter title and authors here): Introduction. Recent reports have identified a consistent reversal of decreasing trends in major lower extremity amputations, with multifactorial drivers from cardiovascular disease to societal and hospital system-based factors.
Research Question. We evaluated if major lower extremity amputation risk differs by hospital Medicaid proportion, socioeconomic status (zip code-based income), and race/ethnicity.
Methods. Using the National Inpatient Sample from 1993 to 2021, we identified inpatient admissions with procedure codes for below-knee (BKA) and above-knee (AKA) amputations. Sample-weighted, population standardized incidence rates per 100,000 people were calculated by hospital Medicaid proportions (defined as quantiles with increasing proportions), zip code-based income quartile, and race/ethnicity. Landmark analyses using multivariable logistic regressions – with inflection points identified in previous amputation incidence analyses at 2010 for BKA and 2012 for AKA – evaluated associations between amputation risk, hospital Medicaid proportion quantile, income quartile, and race/ethnicity.
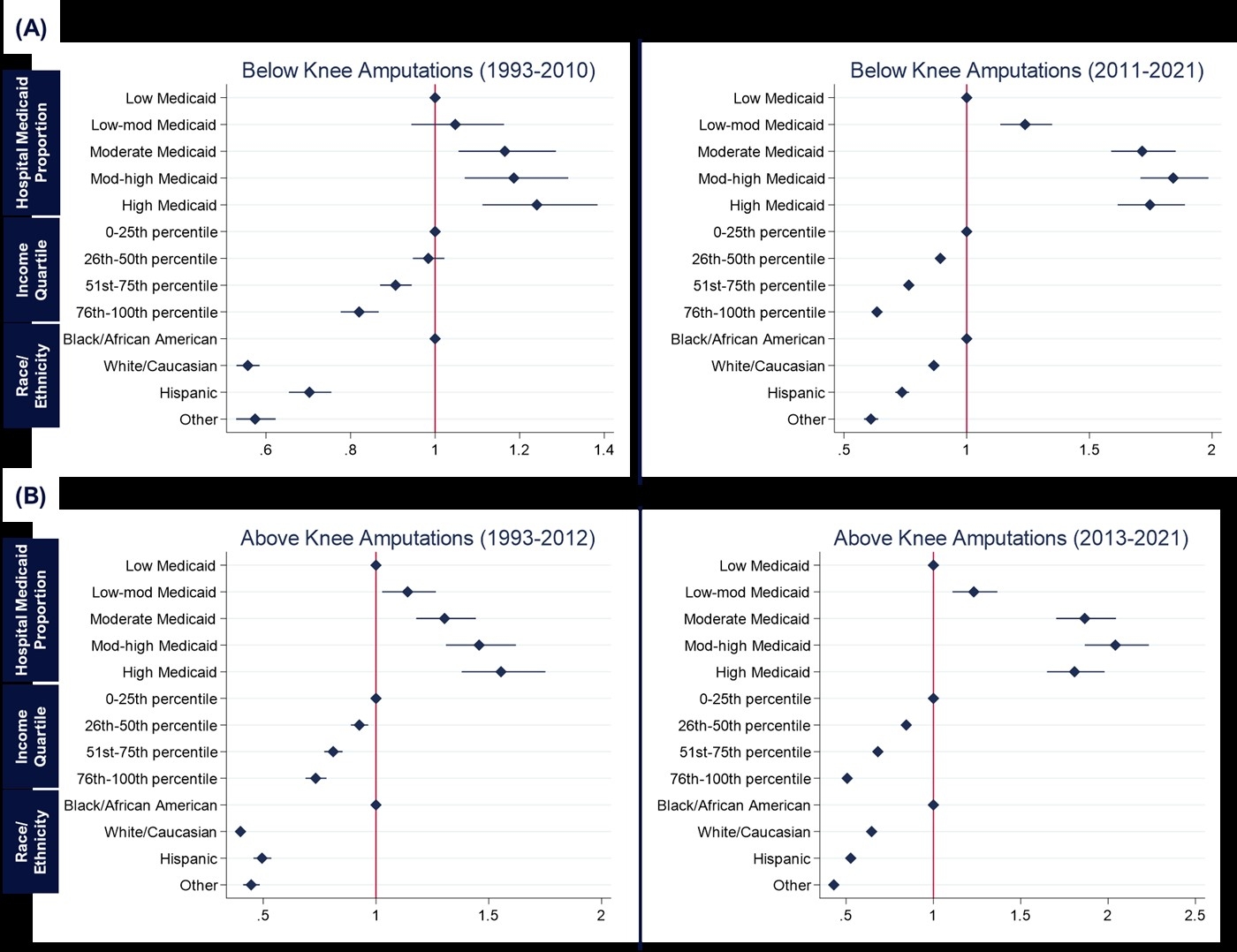
Results. In a sample of 2,769,388 admissions, 197,018 (7.1%) had BKA and 151,018 (5.5%) had AKA. Almost 50% of major amputations were performed in the highest Medicaid proportion facilities. Similarly, 38% of amputations, both AKA and BKA, were reported in the lowest income quartile. Pre-inflection points, for both AKA and BKA, we observed a clear, linearly increasing risk association between higher hospital Medicaid proportion, lower income, and being Black with amputations (Figure). Post-inflection, an elevated risk remained and was distributed relatively equally among hospitals with higher Medicaid proportions (BKA odds ratio [OR]: 1.71, 1.84, 1.75; AKA OR: 1.87, 2.04, 1.81; all p<0.001). For income, there was a widening gap with progressively greater risk in lower quartiles (BKA OR: 1.71, 1.84, 1.75; AKA OR: 1.87, 2.04, 1.81; all p<0.001).
Conclusions. Pre-inflection, high amputation risk was concentrated in extreme settings. After amputation incidence increased (i.e., post-inflection), amputation burden now spans more hospital systems and profoundly impacts lower income groups - representing changing hospital and societal risk characteristics. These findings emphasize targeting and optimizing care at high-risk hospitals and patients.
Sharath, Sherene
(
SUNY Downstate Health Sciences Uni
, Brooklyn , New York , United States )
Natarajan, Sundar
(
NYU School of Medicine
, New York , New York , United States )
Sihaloho, Dewi
(
SUNY Downstate Health Sciences Uni
, Brooklyn , New York , United States )
Ferguson, Claire
(
SUNY Downstate Health Sciences Uni
, Brooklyn , New York , United States )
Medvedovsky, Steven
(
SUNY Downstate Health Sciences Uni
, Brooklyn , New York , United States )
Kougias, Panos
(
SUNY Downstate Health Sciences Uni
, Brooklyn , New York , United States )
Author Disclosures:
Sherene Sharath:DO NOT have relevant financial relationships
| Sundar Natarajan:DO NOT have relevant financial relationships
| Dewi Sihaloho:DO NOT have relevant financial relationships
| Claire Ferguson:DO NOT have relevant financial relationships
| Steven Medvedovsky:DO NOT have relevant financial relationships
| Panos Kougias:DO NOT have relevant financial relationships