Noninvasive Respiratory Support After Cardiothoracic Surgery: A Network Meta-analysis
Abstract Body (Do not enter title and authors here): Background Cardiothoracic surgery is associated with a high incidence of postoperative respiratory complications arising from a combination of patient-related and procedural risk factors. Although noninvasive respiratory support strategies, including high-flow nasal cannula (HFNC), noninvasive positive pressure ventilation (NIPPV), and conventional oxygen therapy (COT), are commonly used to reduce post-extubation complications, their relative effectiveness in this population remains uncertain.
Methods We conducted a comprehensive search of Embase, PubMed, and Scopus between January 2010 and December 2024 to identify randomized controlled trials that compared the efficacy of HFNC, COT and NIPPV in adult patients following CTS. A frequentist network meta-analysis was performed. Outcomes included reintubation rate, in-hospital mortality, ICU and hospital length of stay, pneumonia incidence, CPAP requirement, and PaCO2 levels.
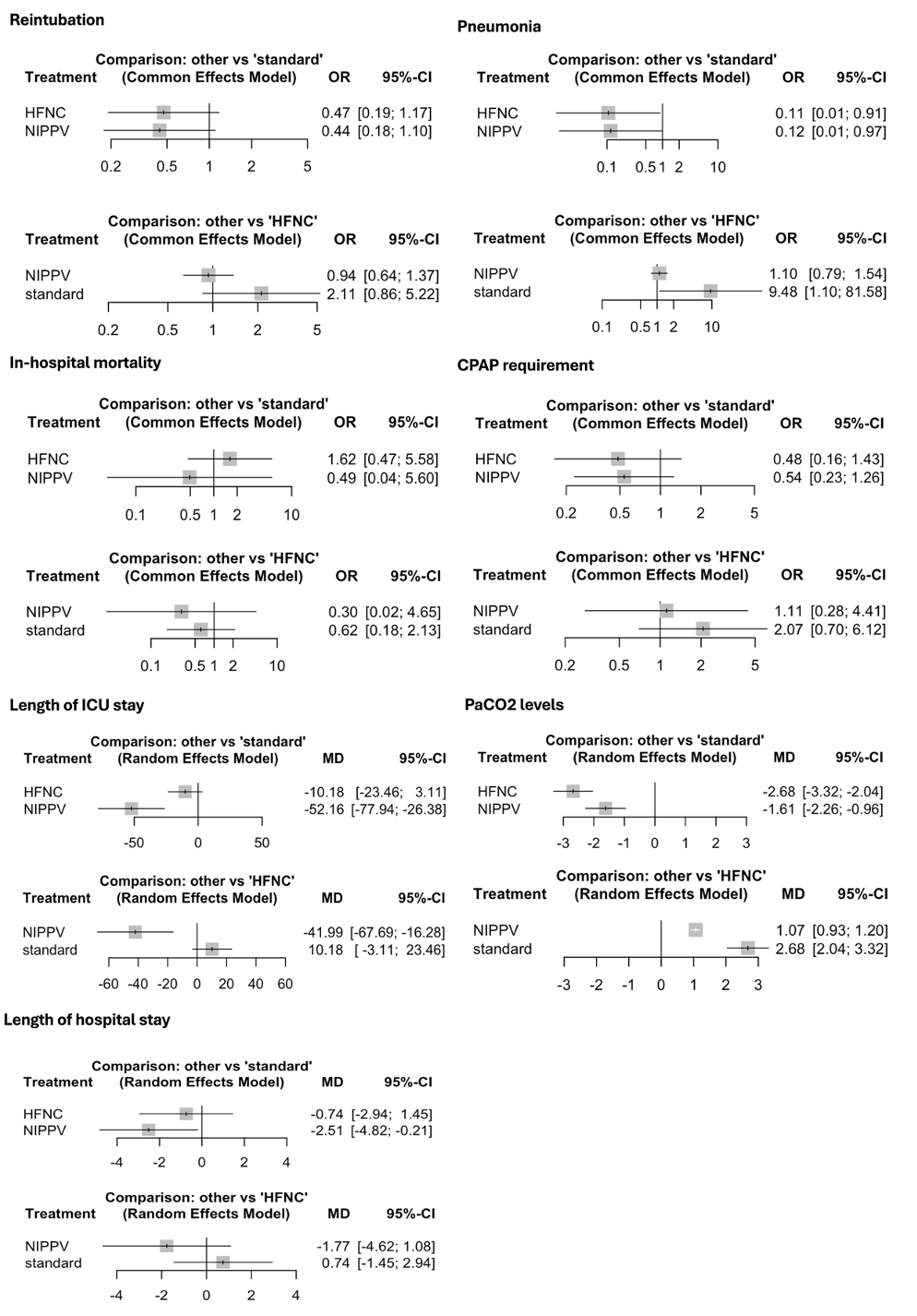
Results Eleven RCTs enrolling 1,664 patients were analyzed. There were no statistically significant differences in reintubation rates, in-hospital mortality, or CPAP requirements between HFNC and COT, NIPPV and COT, or NIPPV and HFNC. NIPPV significantly reduced ICU length of stay compared to both COT (MD –52.16 hours; 95% CI, –77.94 to –26.38) and HFNC (MD –41.99 hours; 95% CI, –67.69 to –16.28), and also shortened hospital length of stay compared to COT (MD –2.51 days; 95% CI, –4.82 to –0.21). Both HFNC and NIPPV were associated with a significantly lower incidence of pneumonia compared to COT (HFNC: OR 0.11; 95% CI, 0.01 to 0.91; NIPPV: OR 0.12; 95% CI, 0.01 to 0.97). In terms of PaCO2 reduction, both HFNC and NIPPV significantly lowered levels compared with COT (HFNC: MD –2.68 mmHg; 95% CI, –3.32 to –2.04; NIPPV: MD –1.61 mmHg; 95% CI, –2.26 to –0.96), with HFNC showing a greater reduction than NIPPV (MD 1.07 mmHg; 95% CI, 0.93 to 1.20).
Conclusion In adult patients undergoing cardiothoracic surgery, the rates of reintubation and in-hospital mortality were similar across noninvasive respiratory support strategies. NIPPV may reduce ICU and hospital length of stay compared with HFNC and COT, while both HFNC and NIPPV may lower the incidence of pneumonia relative to COT. Although these findings support the use of HFNC or NIPPV over COT, the lack of significant differences in key clinical outcomes and overall low certainty of evidence underscores the need for further high-quality randomized trials to clarify their comparative effectiveness.
Nakahara, Shun
(
John A. Burns School of Medicine, University of Hawaii
, Honolulu , Hawaii , United States )
Alexandrino, Francisco
(
Cleveland Clinic Foundation
, Cleveland , Ohio , United States )
Terashima, Rika
(
Stanford University School of Medicine
, Stanford , California , United States )
Miyashita, Satoshi
(
Cleveland Clinic Foundation
, Cleveland , Ohio , United States )
Author Disclosures:
Shun Nakahara:DO NOT have relevant financial relationships
| Francisco Alexandrino:No Answer
| Rika Terashima:DO NOT have relevant financial relationships
| Satoshi Miyashita:No Answer