Milrinone Associated with Lower Mortality and Higher Arrhythmia Risk in Comparison to Dobutamine in End-Stage Heart Failure Without Renal Dysfunction
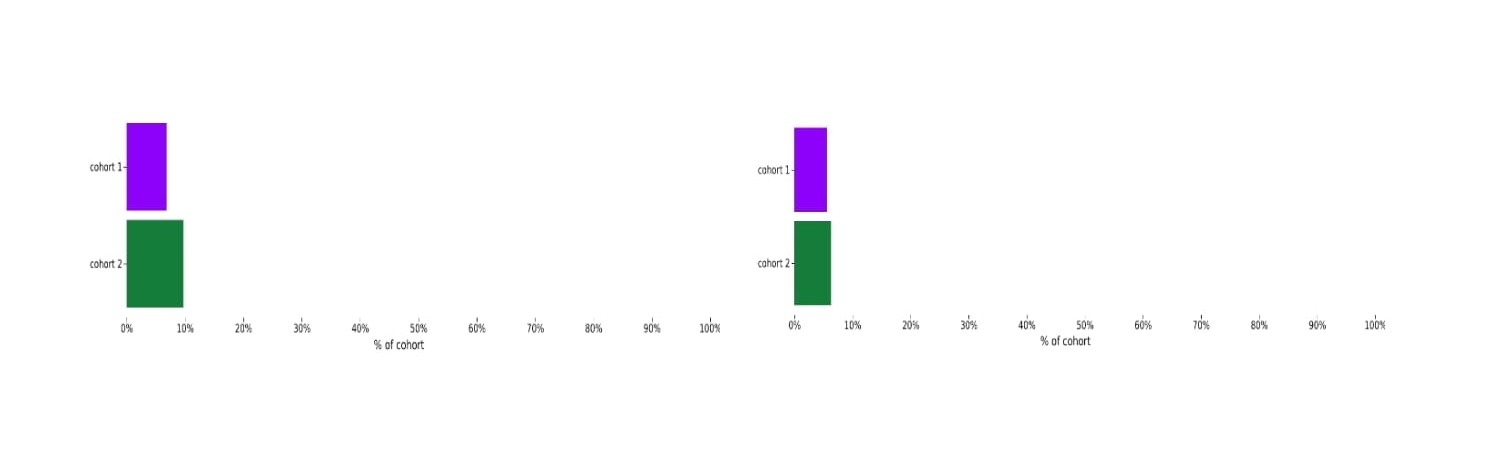
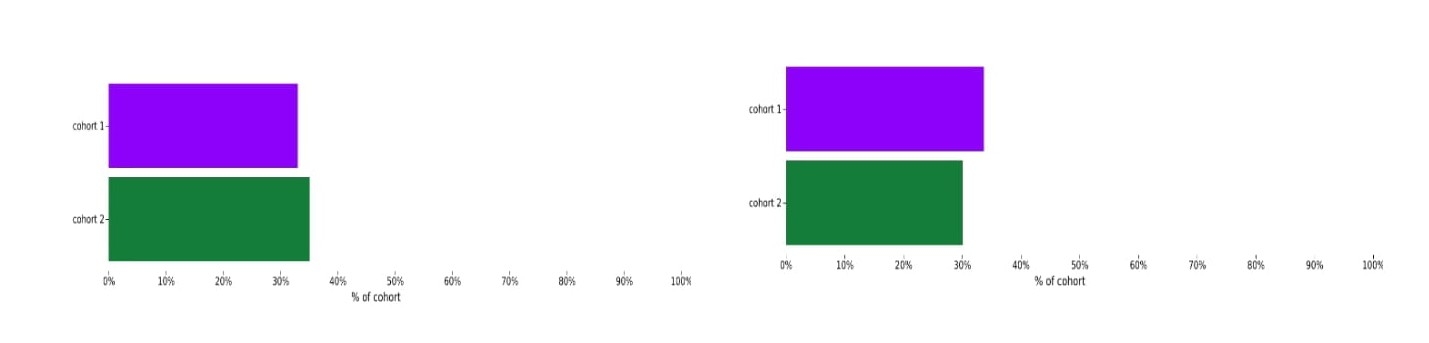
Abstract Body (Do not enter title and authors here): Introduction: Milrinone and dobutamine are commonly used inotropes for advanced heart failure, but comparative data in patients without renal dysfunction are limited. Prior studies rarely focus on this subgroup and often lack real-world representation or adjustment for comorbidities and lab parameters. This study uses a multi-institutional, real-world database to compare short- and long-term outcomes of these agents in patients with end-stage heart failure and preserved renal function. Hypothesis: In patients with end-stage heart failure and preserved renal function, milrinone use is associated with lower mortality but a differing arrhythmia risk compared to dobutamine. Methods: We conducted a retrospective cohort study using the TriNetX Research Network. Hospitalized patients with end-stage heart failure who received either milrinone or dobutamine were included. Exclusions were: use of both agents during index hospitalization, eGFR <60, AKI, CKD stage 3–5, prior transplant, mechanical circulatory support, or documented palliative care. Propensity score matching (1:1) was applied across demographics, comorbidities, medications, and lab/clinical parameters. Outcomes included all-cause mortality and atrial/ventricular arrhythmias over 30-day, 1-year, and 5-year windows. Patients were excluded from each outcome analysis if the outcome occurred prior to the index event. Results: Post-matching, 6,051 patients were included per cohort. Thirty-day mortality was lower with milrinone (414/6,035) than dobutamine (587/6,014), RR 0.703 (95% CI: 0.623–0.793). At 1 year, mortality was 1,159 vs. 1,378 (RR 0.838; 95% CI: 0.782–0.898). At 5 years, mortality was 1,993 vs. 2,110 (RR 0.941; 95% CI: 0.896–0.989). Milrinone was associated with higher arrhythmia incidence at 1 year (RR 1.125; 95% CI: 1.008–1.255) and 5 years (RR 1.121; 95% CI: 1.036–1.212), but not at 30 days. Conclusion: In patients with end-stage heart failure and preserved renal function, milrinone was associated with lower all-cause mortality but increased arrhythmia risk over longer follow-up. These findings indicate that there may be underlying outcome differences between inotropic choices for certain patient populations, and prospective trials are warranted.
Singh, Gurkaranvir
(
Creighton University School of Medicine Phoenix
, Phoenix , Arizona , United States )
Bharaj, Inderjeet Singh
(
Abrazo Healthcare
, Glendale , Arizona , United States )
Saririan, Mehrdad
(
Creighton university Phoenix
, Phoenix , Arizona , United States )
Rohant, Namit
(
Creighton university Phoenix
, Phoenix , Arizona , United States )
Singh, Sandeep
(
Indiana University
, Indianapolis , Indiana , United States )
Author Disclosures:
Gurkaranvir Singh:DO NOT have relevant financial relationships
| Inderjeet Singh Bharaj:DO NOT have relevant financial relationshipsNamit Rohant:No Answer
| Sandeep Singh:No Answer