Takayasu arteritis presenting as hemorrhagic cerebrovascular accident
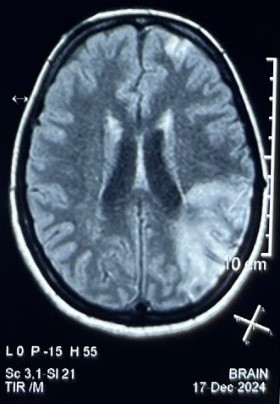
Abstract Body (Do not enter title and authors here): Description: A 24-year-old female presented to the emergency department with acute onset of right-sided hemiparesis accompanied by right facial drooping. Neurological examination revealed a GCS of 15/15, a positive right Babinski sign, diminished right-sided tone, and early-stage flaccid paralysis on the right. A left lower motor neuron-type facial palsy affecting only the lower half of the face was noted, with sparing of the forehead. Pulse examination demonstrated asymmetric peripheral pulses: non-palpable radial pulses in the right upper limb and faint peripheral pulses in the left upper limb. Blood pressure recorded in the left lower extremity (140/80 mmHg), followed by the right lower extremity (120/70 mmHg) and left upper limb (95/60 mmHg) and unrecordable in the right upper limb. Bilateral carotid bruits were auscultated. The patient had no prior history of CVA. Investigations: CEMRI BRAIN showed subacute infarct with hemorrhagic transformation in left parietal, temporal and occipital lobe, subacute infarct in left frontal lobe, foci of FFE in blooming in anterior limb of right and posterior limb of left internal capsule.CT angiography revealed diffuse mural thickening in the aortic arch,ascending and descending aorta, marked narrowing in the brachiocephalic artery and both common carotids, with saccular aneurysms, attenuation of intracranial ICA, ACA, and MCA, particularly on the right side. Disscussion: Neurological involvement in Takayasu arteritis is relatively common and ischemic strokes have been documented in approximately 10–20% of patients. In contrast, hemorrhagic cerebrovascular accidents are exceedingly rare in Takayasu arteritis. When aneurysms are located intracranially or in cervical vessels, they can rupture and lead to subarachnoid or parenchymal hemorrhages. In rare case reports, patients have presented with subarachnoid hemorrhage or lobar intracerebral hemorrhage, with imaging consistent with TA. Given the rarity of this, diagnosis is frequently delayed or missed, especially in young individuals without classic risk factors for stroke. A high index of suspicion is necessary when patients present with stroke-like symptoms in conjunction with signs of large-vessel disease—such as vascular bruits, diminished pulses, or unexplained blood pressure asymmetry. In hemorrhagic cases, aggressive blood pressure control is essential to prevent rebleeding, and the role of interventional neurosurgery is guided by aneurysmal size and location.
Sharma, Karan
(
Gmch, Chandigarh
, Chandigarh , India )
Gupta, Monica
(
Gmch, Chandigarh
, Chandigarh , India )
Khetarpal, Mehak
(
Gmch, Chandigarh
, Chandigarh , India )
Author Disclosures:
Karan Sharma:No Answer
| Monica Gupta:No Answer
| Mehak Khetarpal:DO NOT have relevant financial relationships