Indirect Echocardiographic Markers of Procedural Success in Mitral Transcatheter Interventions: A Case Series
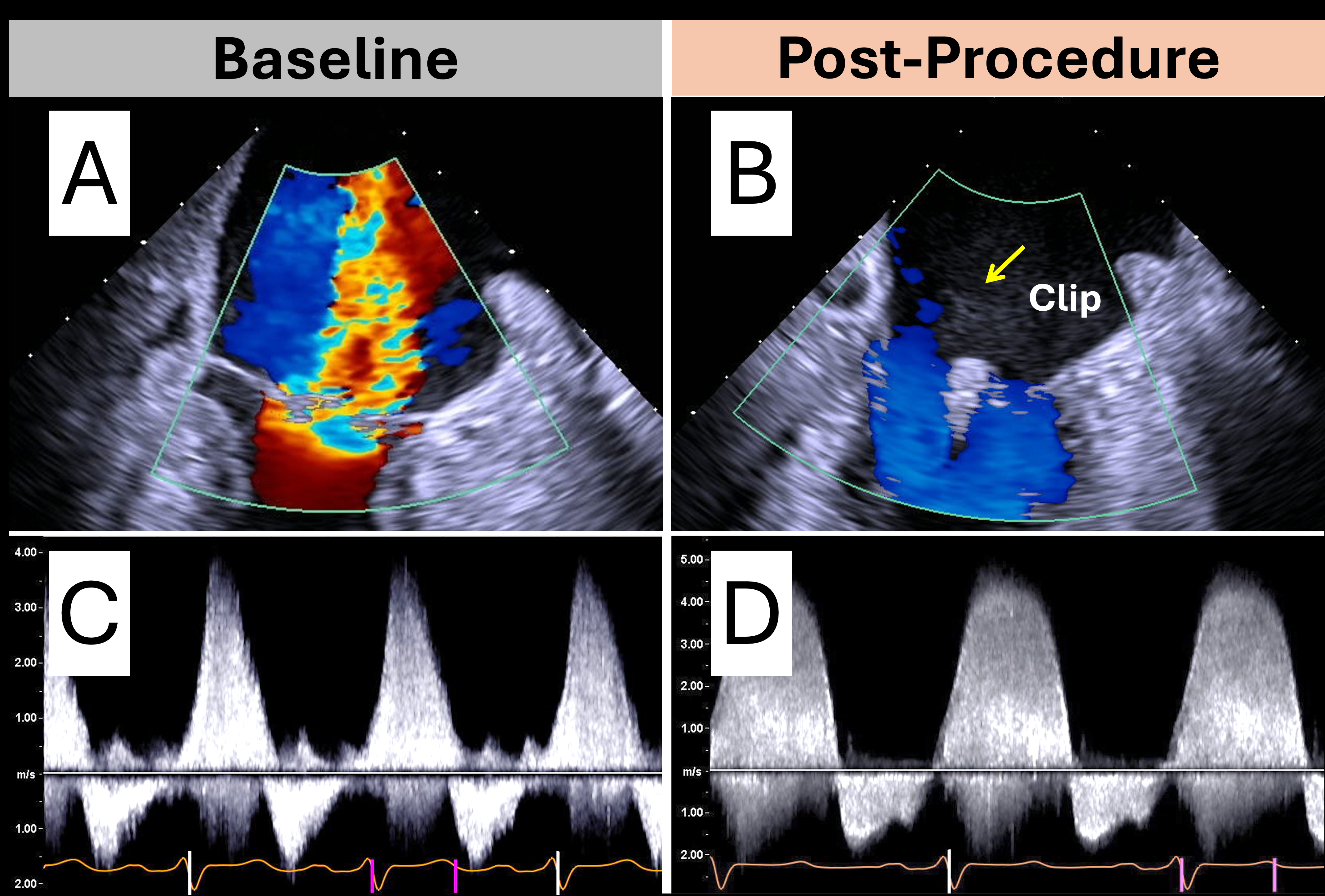
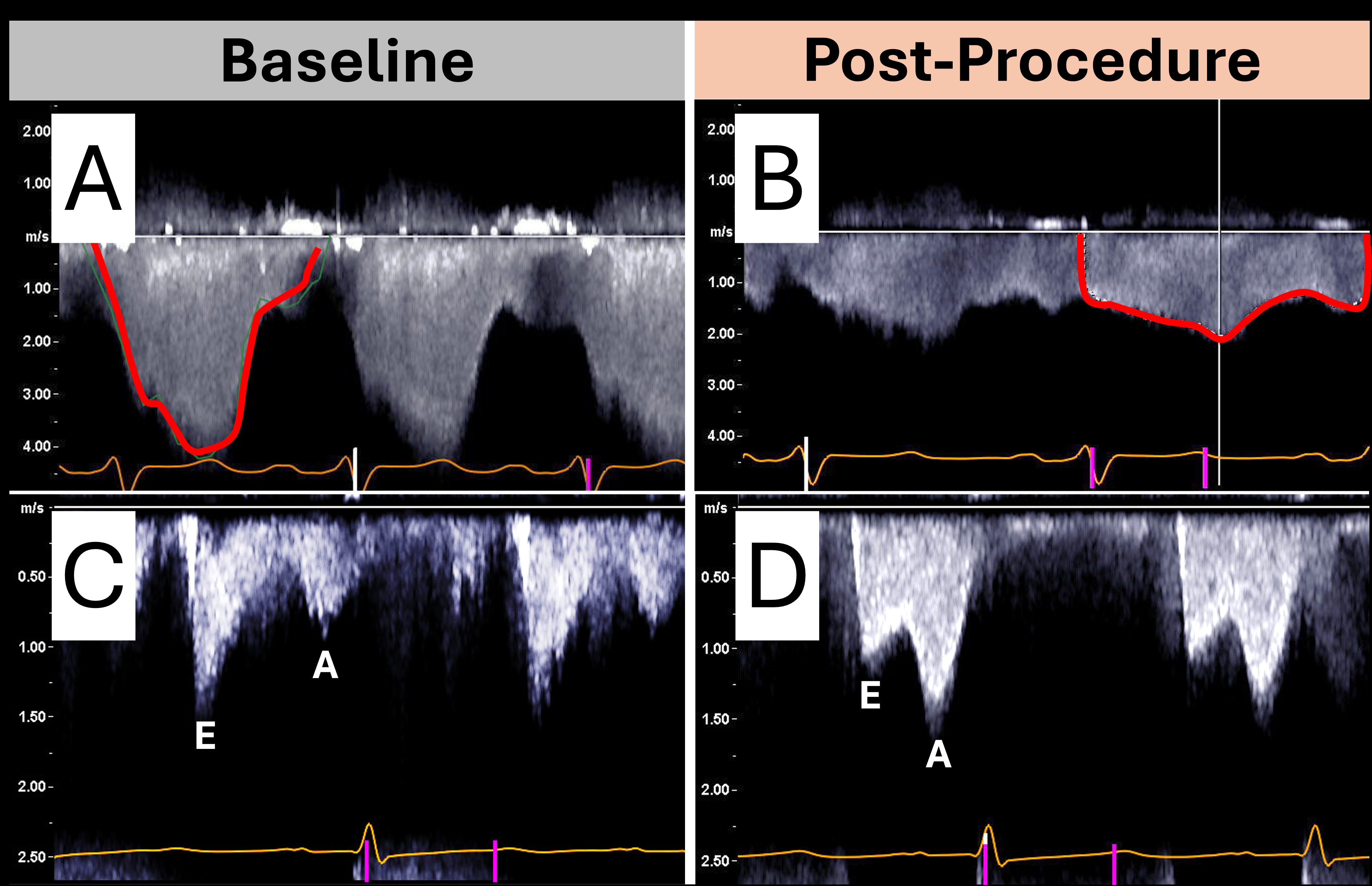
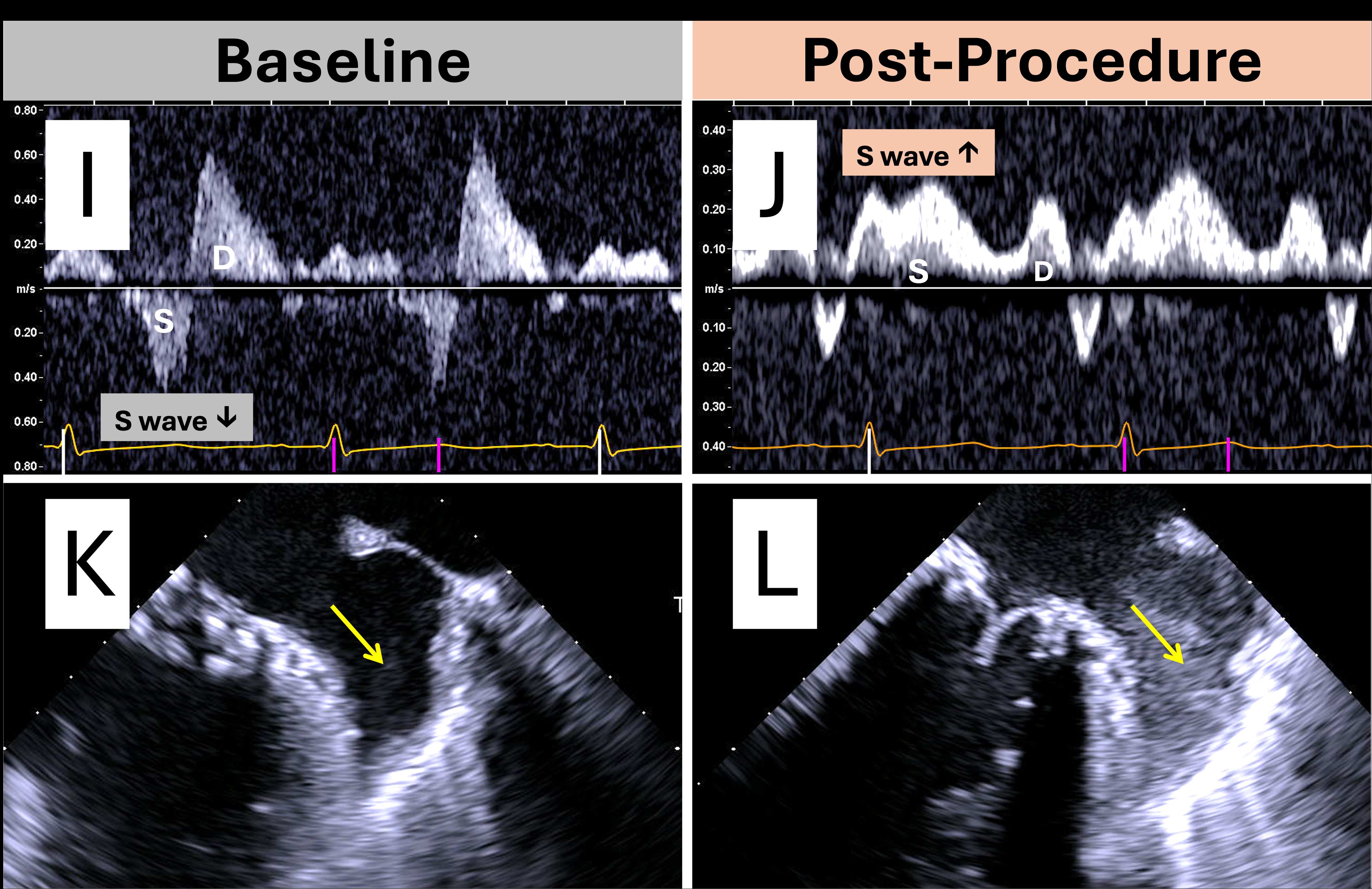
Abstract Body (Do not enter title and authors here): Introduction: Standard echocardiographic measures of mitral regurgitation (MR) severity, such as vena contracta width (VCW) and effective regurgitant orifice area (EROA), are often unreliable after transcatheter mitral interventions due to altered valve anatomy. This case series highlights indirect echocardiographic parameters that collectively aid in assessing successful MR reduction after mitral interventions such as transcatheter edge-to-edge repair (TEER). Case Descriptions: Case 1: An 80-year-old woman with severe degenerative MR had a large, central MR jet occupying most of the left atrium (LA) and an LVOT stroke volume of 31 mL. Post-TEER, the MR jet resolved and LVOT stroke volume rose to 53 mL. Case 2: A 53-year-old man with severe functional MR had a dense, early-peaking with low-Vmax, triangular MR jet on spectral Doppler and a peak/mean iatrogenic atrial septal defect (ASD) gradient of 72/28 mm Hg. Post-TEER, the MR jet became parabolic with low Vmax and less dense, and the ASD gradient dropped to 16/9 mm Hg. Case 3: An 82-year-old woman with degenerative MR showed an E-wave dominant mitral inflow pattern with slow deceleration and pulmonary S wave reversal in the right upper pulmonary vein (RUPV). After TEER, the inflow pattern became A-wave dominant, and S wave reversal resolved. Case 4: A 54-year-old woman with chronic atrial fibrillation and severe MR after surgical valve replacement showed no spontaneous echo contrast (SEC) in the left atrial appendage (LAA). After valve-in-valve (ViV), there is now persistence of SEC. Discussion: Key echocardiographic indicators of resolved severe MR post-intervention include: (1) marked reduction in jet area on color Doppler, (2) increased LVOT stroke volume indicating improved forward flow, (3) transition from a dense, low-Vmax, triangular MR jet contour to a less dense, high Vmax, parabolic MR jet contour on spectral Doppler reflecting improved LA hemodynamics, (4) decreased transseptal pressure gradient across the iatrogenic ASD reflecting improved LA pressure, (5) shift from E-wave to A-wave dominant mitral inflow in the absence of significant mitral stenosis, (6) return of antegrade pulmonary S wave flow reflecting decreased LA pressure, and (7) reappearance of LAA SEC, as the MR jet no longer washes away the SEC seen in chronic atrial fibrillation. While no single measure is definitive, these findings support a multimodal approach to residual MR assessment and highlight the need for further validation.
Asachi, Parsa
(
NYU Langone Health
, New York , New York , United States )
Freedberg, Robin
(
NEW YORK UNIV SCHOOL MED
, New York , New York , United States )
Ro, Richard
(
NYU Langone Health
, New York , New York , United States )
Bamira, Daniel
(
NYU-Langone Health
, New York , New York , United States )
Vainrib, Alan
(
NYU Langone Health
, New York , New York , United States )
Saric, Muhamed
(
New York University
, New York , New York , United States )
Author Disclosures:
Parsa Asachi:DO NOT have relevant financial relationships
| Robin Freedberg:No Answer
| Richard Ro:DO NOT have relevant financial relationships
| Daniel Bamira:DO have relevant financial relationships
;
Consultant:Ultrasight:Past (completed)
| Alan Vainrib:No Answer
| Muhamed Saric:DO have relevant financial relationships
;
Speaker:Abbott:Active (exists now)
; Speaker:Medtronic:Active (exists now)
; Speaker:Boston Scientific:Active (exists now)