Trends in United States Mortality Among Patients with Atrial Fibrillation/Flutter-Induced Heart Failure (1999–2024): Disparities by Gender, Race/Ethnicity and Region
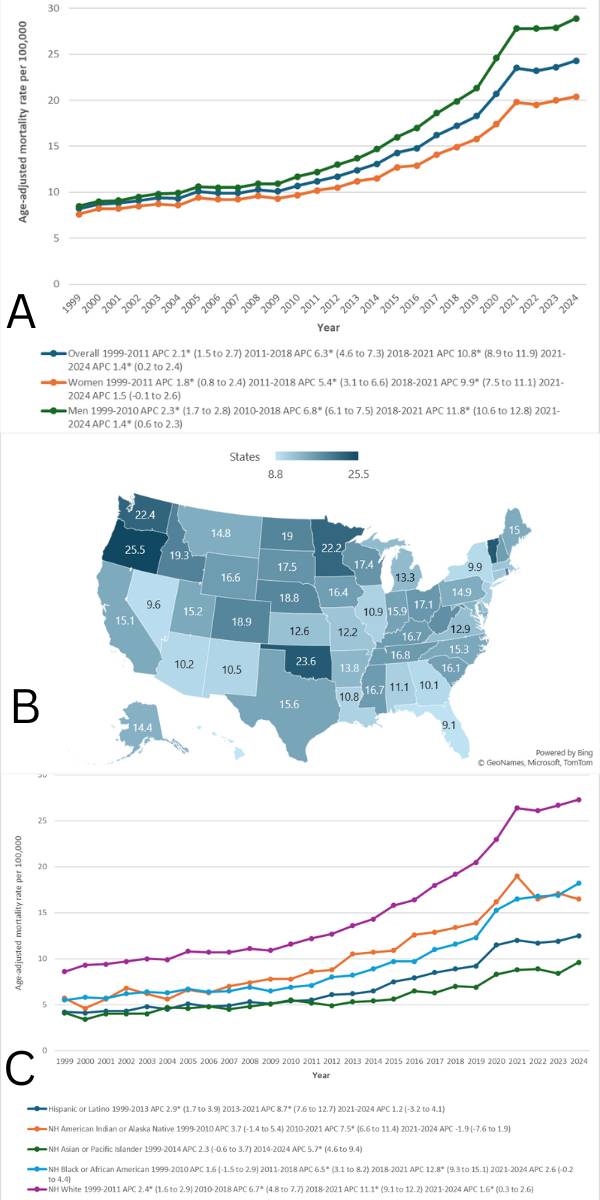
Abstract Body (Do not enter title and authors here): Background: Atrial fibrillation (AF) and heart failure (HF) are prevalent cardiovascular disorders that frequently co-occur, exacerbating each other's effects and resulting in adverse clinical outcomes. Despite the well-established association between these conditions, there is a paucity of research examining AF/atrial flutter (AFL) as direct contributors to HF-related mortality across various demographics and regions within the United States Hypothesis: This study aims to investigate the patterns of AF/AFL-related HF mortality in the U.S. from 1999 to 2024, stratified by age, gender, race/ethnicity, urban-rural classification, and geographic region. Methods: A retrospective analysis was conducted utilizing data from the Centers for Disease Control and Prevention's Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER) database. Mortality data were extracted from death certificates that identified AF/AFL related HF as a primary or contributing cause of death (ICD-10 codes I11.0, I13.0, I13.2, I48 and I50). Age-adjusted mortality rates (AAMRs) per 100,000 individuals were calculated, and annual percentage changes (APC) were assessed using Joinpoint regression. Results: From 1999 to 2024, 1,307,809 deaths in the United States were attributed to atrial fibrillation/flutter-related heart failure (AF/AFL-HF). The age-adjusted mortality rate (AAMR) rose significantly from 8.2 to 24.3 per 100,000. Males consistently had higher AAMRs than females (15.7 vs. 12.3). Racial disparities were evident, with non-Hispanic Whites having the highest cumulative AAMR (15.1), and non-Hispanic Asians/Pacific Islanders the lowest (5.7). Geographic differences were also prominent: Oregon recorded the highest state-level AAMR (25.5), while Hawaii had the lowest (8.8). Regionally, the West (15.3) and Midwest (14.9) had the highest cumulative AAMRs. Place-of-death trends showed a shift toward home deaths, which became the most common location by 2024. Although AAMRs increased sharply from 2010 to 2021 across most subgroups, rates stabilized between 2021 and 2024. Conclusion: AF/AFL-related heart failure mortality has increased substantially over the past 26 years in the U.S. with marked disparities by sex, race/ethnicity, region, and urbanization. While recent years have seen a plateau in mortality rates, the continued burden—especially among vulnerable populations underscores the need for equitable, targeted public health interventions and improved access to cardiovascular care.
., Abdullah
(
Rawalpindi Medical University
, Rawalpindi , Pakistan )
Abdul Malik, Mohammad Hamza Bin
(
Nassau University Medical Center
, East Meadow , New York , United States )
Rani, Suraksha
(
Sir Syed College of Medical Sciences, Pakistan
, Karachi , Pakistan )
Saeed, Humza
(
Rawalpindi Medical University
, Rawalpindi , Pakistan )
Author Disclosures:
Abdullah .:DO NOT have relevant financial relationships
| Mohammad Hamza Bin Abdul Malik:DO NOT have relevant financial relationships
| Suraksha Rani:No Answer
| Laksh Kumar:DO NOT have relevant financial relationships
| Saad Ashraf:No Answer
| Sunaina Bhimani:DO NOT have relevant financial relationships
| Sumet Kumar:DO NOT have relevant financial relationships
| Adarsh Raja:DO NOT have relevant financial relationships
| Humza Saeed:DO NOT have relevant financial relationships
Kumar Laksh, Ihsan Ayesha, Abdul Malik Muhammad Awais Bin, Khan Shahid, Bai Sunanda, Iqbal Faiqa, Naeem Saman, . Abdullah, Abdul Malik Mohammad Hamza Bin
Kumar Laksh, Ullah Irfan, Hafeez Ali Shan, Ali Talha, Ashraf Saad, Sakarwala Aasiya Shahbaz, Zaman Asad, Tagga Muhammad Riyyan, Qureshi Ahmar Jan, Khan Abdul Wali
4357485_File000000.jpg
You have to be authorized to contact abstract author. Please, Login