Colchicine and Cardiovascular Outcomes in Patients With Coronary Artery Disease and Elevated C Reactive Protein
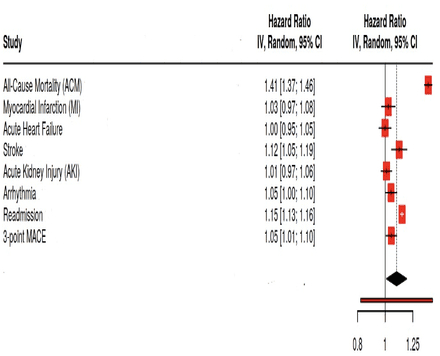
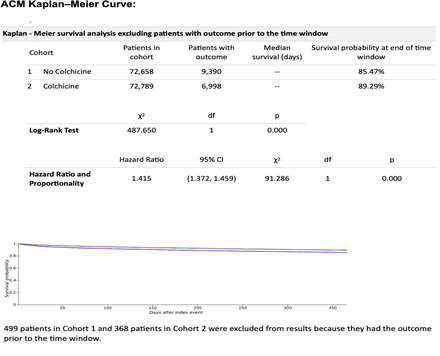
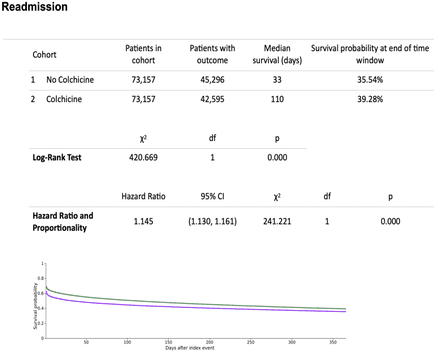
Abstract Body (Do not enter title and authors here): Background: Colchicine, an anti-inflammatory agent, has been investigated for reducing cardiovascular risk in patients with atherosclerotic coronary artery disease (CAD). This study assessed 1-year clinical outcomes in CAD patients with elevated C-reactive protein (CRP), comparing those untreated with colchicine to those who received it. Research Hypothesis: We hypothesized that colchicine use would reduce adverse cardiovascular outcomes over one year in this high-risk population. Goals: To compare 12-month clinical outcomes between colchicine-treated and untreated CAD patients with elevated CRP. Methods: A retrospective cohort study was conducted using the TriNetX Research Network. Adults with atherosclerotic heart disease and CRP 2.5–999 mg/L were included. Two cohorts were defined: patients without colchicine exposure (Cohort 1, n=73,157) and those prescribed colchicine (Cohort 2, n=73,157), matched 1:1 using propensity scores. Matching was performed on demographic and comorbidity variables including age, sex, race/ethnicity, and clinical diagnoses such as heart failure, CKD, AF, HTN, obesity, diabetes, PVD, COPD, and liver disease. Covariate balance was assessed using standardized mean differences (SMD), with SMD <0.1 indicating adequate balance. Analyses used TriNetX Analytics. Outcomes at 12 months included all-cause mortality (ACM), myocardial infarction (MI), stroke, acute heart failure, acute kidney injury (AKI), arrhythmia, hospital readmission, and 3-point major adverse cardiovascular events (MACE). Results: Compared to colchicine-treated patients, those not receiving colchicine had significantly higher hazard of ACM (HR 1.415; 95% CI: 1.372–1.459; p<0.001), stroke (HR 1.119; 95% CI: 1.051–1.193; p=0.001), arrhythmia (HR 1.048; 95% CI: 1.001–1.099; p=0.047), and 3-point MACE (HR 1.051; 95% CI: 1.006–1.098; p=0.026). No significant differences were observed for MI, heart failure, or AKI. The no-colchicine group had greater risk of hospital readmission (HR 1.145; p<0.001) and shorter median time to readmission (33 vs. 110 days). Conclusion: In this large matched cohort study, CAD patients with elevated CRP not treated with colchicine had significantly higher 1-year mortality and cardiovascular event rates. While causality cannot be inferred due to the observational design, these findings support colchicine’s potential role in secondary prevention and underscore the need for randomized trials.
Dawoud, Abdallatif
(
University of Toledo
, Toledo , Ohio , United States )
Kamel-abusalha, Louie
(
University of Toledo
, Toledo , Ohio , United States )
Bouso, Muhammad
(
Presbyterian Brooklyn Methodist Hospital
, New York , New York , United States )
Soleimani, Hamidreza
(
Tehran University of Medical Sciences
, Tehran , Iran (the Islamic Republic of) )
Khorsand Askari, Mani
(
University of Toledo
, Toledo , Ohio , United States )
Eltahawy, Ehab
(
University of Toledo Medical Center
, Toledo , Ohio , United States )
Author Disclosures:
Abdallatif Dawoud:DO NOT have relevant financial relationships
| Louie Kamel-Abusalha:DO NOT have relevant financial relationships
| Muhammad Bouso:DO NOT have relevant financial relationships
| Hamidreza Soleimani:No Answer
| Mani Khorsand Askari:DO NOT have relevant financial relationships
| Ehab Eltahawy:DO NOT have relevant financial relationships