Postprocedural Anticoagulation Following Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction: A Meta-Analysis of Clinical Outcomes
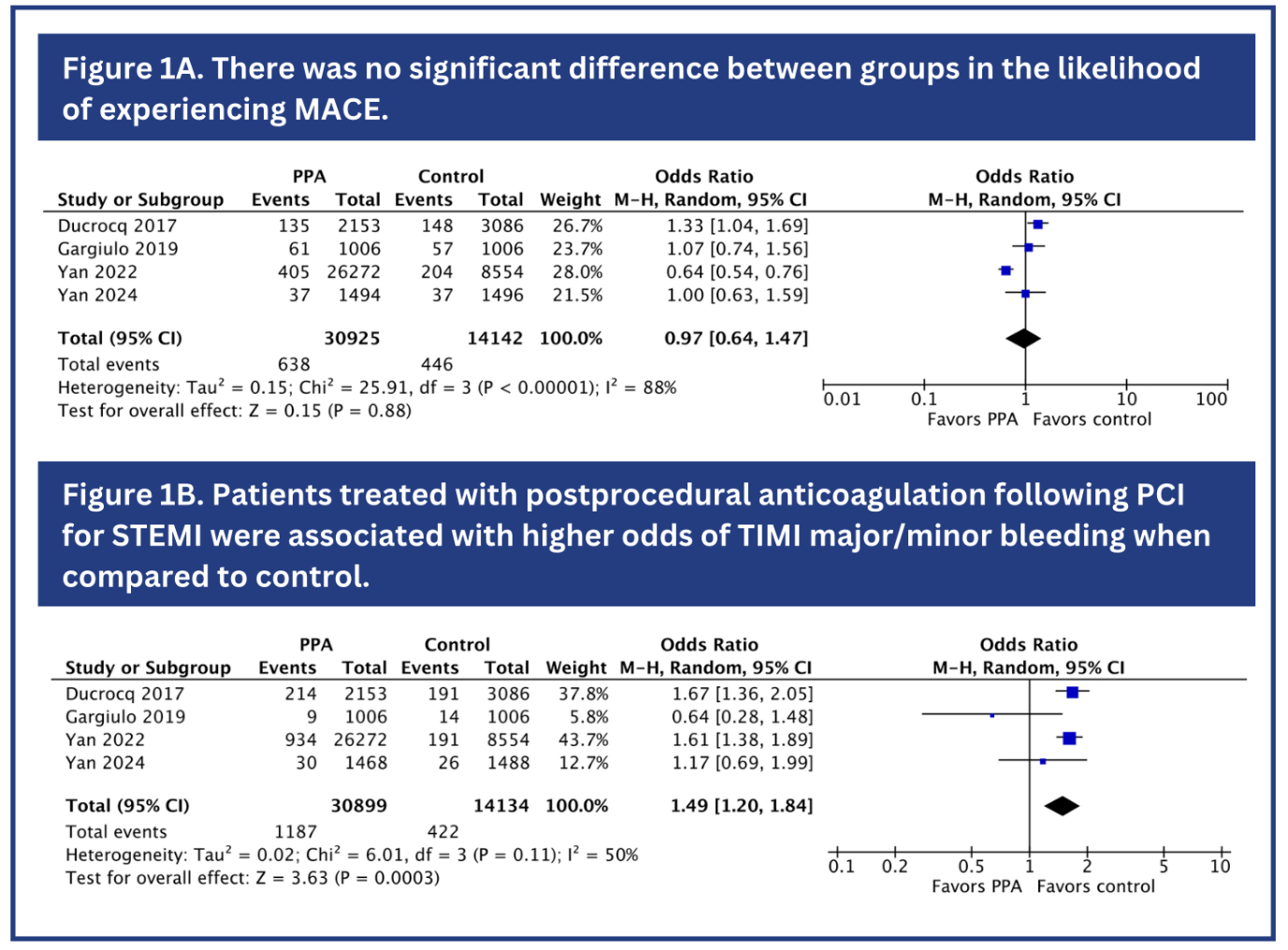
Abstract Body (Do not enter title and authors here): Background: The use of procedural anticoagulation during primary percutaneous coronary intervention (PCI) is well established and has been shown to improve clinical outcomes in patients with ST-elevation myocardial infarction (STEMI). Despite its widespread application in clinical settings, the necessity and efficacy of postprocedural anticoagulation (PPA) remain contentious. Thus, this is the first meta-analysis to assess the efficacy and safety of PPA after PCI for the management of STEMI. Methods: A comprehensive search of PubMed, Cochrane, and Embase databases was conducted to identify studies comparing the clinical outcomes between PPA administration and control (placebo or no anticoagulant infusion) following PCI for STEMI treatment. Statistical analyses were performed using RevMan version 5.4.1, employing a random-effects model to calculate odds ratios (ORs) and their 95% confidence intervals (CIs). Results: A total of four studies comprising 45,066 patients were included (2 RCTs and 2 non-randomized studies), of which 30,925 (68.6%) received PPA. Among the included patients, 35,770 (79.4%) were female. Compared to the control group, PPA did not significantly reduce all-cause mortality (OR 0.82; 95% CI 0.49 – 1.36; P=0.44), cardiac death (OR 0.81; 95% CI 0.49 – 1.33; P=0.41), and major adverse cardiovascular events (MACE) (OR 0.97; 95% CI 0.64 – 1.47; P=0.88; Figure 1A). Moreover, the odds of stent thrombosis (OR 1.24; 95% CI 0.92 – 1.68; P=0.15), myocardial infarction (OR 1.03; 95% CI 0.79 – 1.36; P= 0.81) and stroke (OR 0.95; 95% CI 0.41 – 2.20; P=0.90) did not differ between the groups. However, patients receiving PPA were associated with higher odds of TIMI major/minor bleeding (OR 1.49; 95% CI 1.20 – 1.84; P<0.01; Figure 1B). Conclusions: This meta-analysis reveals no significant differences in the odds of all-cause mortality, cardiac death, MACE, stent thrombosis, myocardial infarction and stroke between PPA and control following PCI for the management of STEMI. However, PPA was associated with higher odds of TIMI major/minor bleeding when compared to control. Further randomized controlled trials are warranted to corroborate these findings.
Oliveira, Vinicius
(
Federal University of Goiás
, Goiânia , Goiás , Brazil )
Gaban, Natalia
(
Federal university of Mato Grosso
, Campo Grande , Brazil )
Silva, Ariadne
(
Evangelical University of Goiás
, Anápolis , Goiás , Brazil )
Lopes, Lucca
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Alves Alencar, Pedro Lucas
(
Federal University of Goiás
, Goiânia , Goiás , Brazil )
Duarte Lima, Ana Paula
(
University of Rio Verde
, Rio Verde , Goiás , Brazil )
Oliveira, Izadora
(
Federal University of Goiás
, Goiânia , Goiás , Brazil )
Graner Moreira, Humberto
(
Federal University of Goiás
, Goiânia , Goiás , Brazil )
Author Disclosures:
Vinicius Oliveira:DO NOT have relevant financial relationships
| Natalia Gaban:No Answer
| ARIADNE SILVA:No Answer
| Lucca Lopes:DO NOT have relevant financial relationships
| Pedro Lucas Alves Alencar:DO NOT have relevant financial relationships
| Ana Paula Duarte Lima:No Answer
| Izadora Oliveira:DO NOT have relevant financial relationships
| Humberto Graner Moreira:No Answer
Witteles Ronald, Mitter Sumeet, Gillmore Julian, Hanna Mazen, Berk John, Mitchell Joshua, Shah Keyur, Kobayashi Masatake, Xiong Kuangnan, Castano Adam, Tamby Jean-francois, Fox Jonathan
Oliveira Izadora, Graner Moreira Humberto, De Sousa Andre, Paiva Arthur, Ferreira Vitor, De Sá Carlos Eduardo, Alves Alencar Joao Victor, Alves Alencar Pedro Lucas, Duarte Lima Ana Paula, Oliveira Vinicius