Risk for appropriate ICD intervention and complications in patients implanted after an out-hospital cardiac arrest compared to patients implanted for primary and other secondary prevention indication
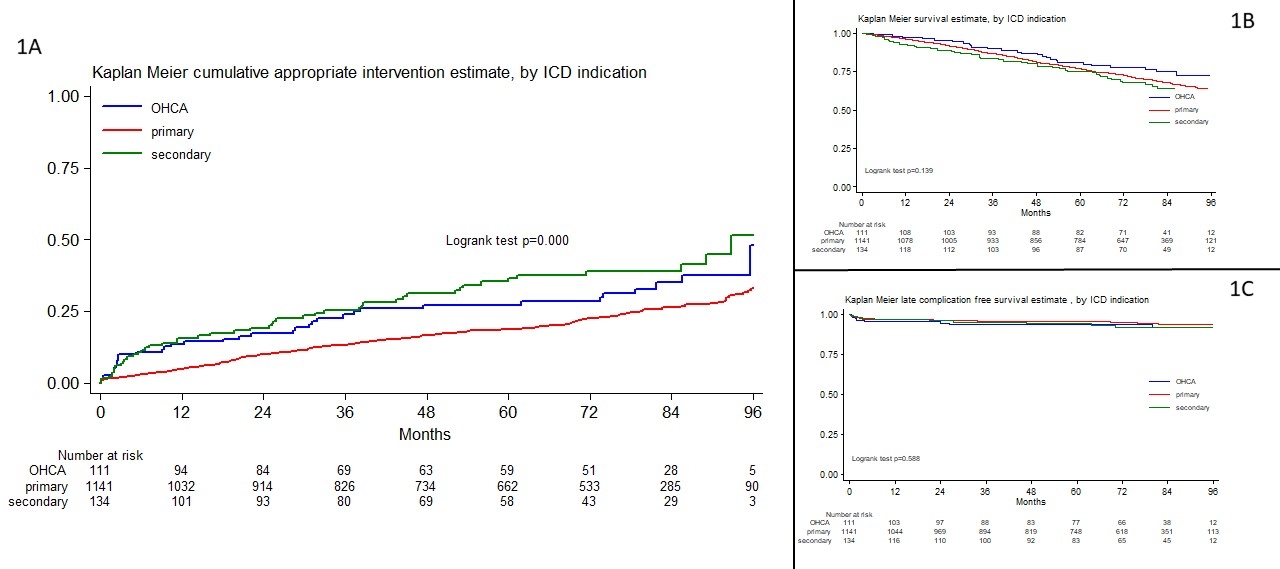
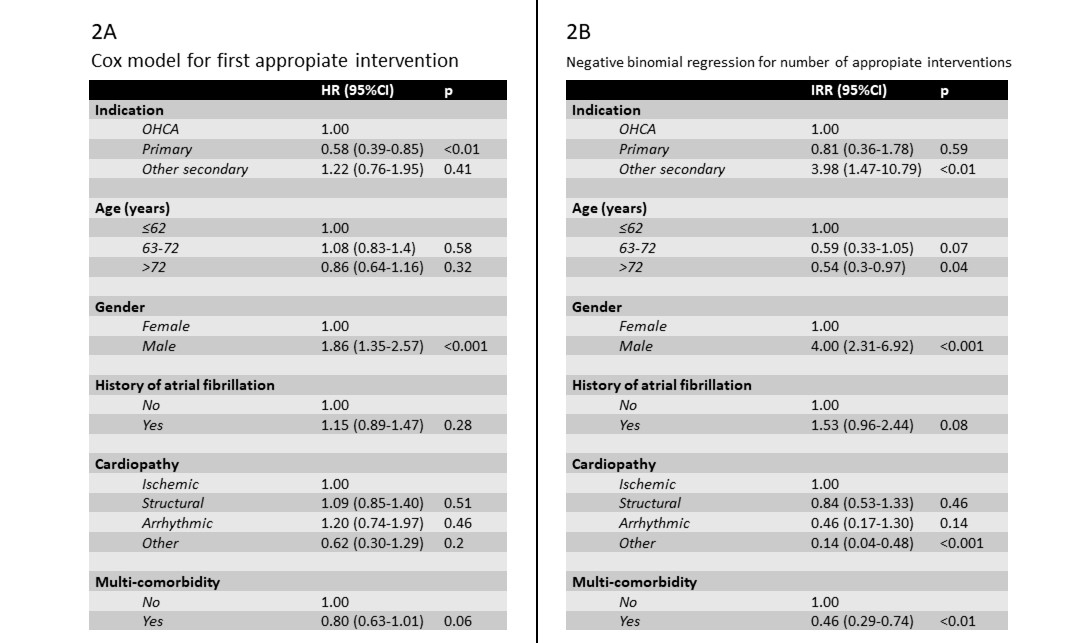
Abstract Body (Do not enter title and authors here): Background: it is unclear if patients implanted with an implantable cardioverter defibrillator (ICD) after an out-of-hospital cardiac arrest (OHCA) have a higher risk of appropriate device therapy than patients implanted for primary and other secondary prevention. Aims: to assess if appropriate device interventions (ATP/shocks) are higher in patients implanted after OHCA compared to patients implanted for primary and secondary prevention other than OHCA. To verify also if mortality, implantation-related complications (pneumothorax, hemothorax, hematoma, cardiac tamponade), device-related complications (lead displacement and fracture, infections) and inappropriate shocks/ATP are higher in OHCA patients. Methods: a retrospective multicenter international study. We included all the patients implanted with an ICD in 2015 and 2016 in the centers. Follow-up was concluded if death or at the last follow-up available until 12/2023. Patients were divided according to ICD indication (secondary prevention after OHCA, other secondary prevention, primary prevention). Results: 1386 patients (79% males; median age 67, IQR 59-74) from 15 centers were included (median follow-up 83 months): 111 patients in OHCA group, 134 in other secondary prevention group and 1141 in primary prevention group. Considering the first appropriate intervention, a significant difference among the three groups was observed (Fig.1A) and, at post-hoc comparison, the OHCA group was at higher risk than primary prevention (HR 1.51, 95%CI 1.06-2.17, p=0.02), but was at similar risk than other secondary prevention (HR 0.79, 95%CI 0.51-1.23, p=0.3). This was confirmed also after correction for age, gender, history of atrial fibrillation, aetiology and multi-comorbidity (Fig.2A). Considering the number of appropriate interventions during follow-up, the risk of OHCA group was lower than other secondary prevention (IRR 0.28, 95%CI 0.11-0.68, p<0.01) and similar to primary prevention (IRR 0.97, 95%CI 0.47-1.96, p=0.93), also after correction for the other predictors (Fig.2B). The three groups showed no differences in survival (Fig.1B), implantation-related complication, device-related complications (Fig.1C) and inappropriate shocks/ATP. Conclusion: Our study highlights how OHCA patients represents a peculiar population with the same chance of survival and rate of complications compared to primary and other secondary prevention patients suggesting the need of more studies to improve their long-term treatment.
Enrico Baldi:DO NOT have relevant financial relationships
| Veronica Dusi:DO NOT have relevant financial relationships
| Valentina Guerini Giusteri:No Answer
| Pasquale Crea:DO NOT have relevant financial relationships
| Nicolo Martini:DO NOT have relevant financial relationships
| Federico Guerra:No Answer
| Lucy Barone:DO NOT have relevant financial relationships
| Vincenzo Russo:DO NOT have relevant financial relationships
| Stefano Cornara:DO NOT have relevant financial relationships
| Roberto Rordorf:DO NOT have relevant financial relationships
| catherine klersy:No Answer
| Antonio Curcio:DO NOT have relevant financial relationships
| simone savastano:DO NOT have relevant financial relationships
| Martina Nesti:No Answer
| Pietro Palmisano:No Answer
| Gianmarco Arabia:No Answer
| Gabriele Dell'Era:No Answer
| Matteo Casula:DO NOT have relevant financial relationships