Invasive Hemodynamic Validation of a Novel Echocardiographic Artificial Intelligence Screening Tool for HFpEF
Abstract Body (Do not enter title and authors here): Background: Right heart catheterization (RHC) is the gold standard for diagnosing heart failure with preserved ejection fraction (HFpEF). An FDA-approved artificial intelligence (AI) technology uses a four-chamber transthoracic echocardiogram (TTE) image to screen patients for HFpEF.
Methods: We compared invasive hemodynamic data between patients screened for HFpEF by this TTE AI algorithm. We retrospectively collected data from two cohorts of patients with an ejection fraction (EF) ≥ 50% undergoing RHC for the evaluation of HFpEF. The most recent TTE was screened using the AI tool and reported as either suggestive or non-suggestive for HFpEF – labeled as “positive” or “negative,” respectively. Invasive hemodynamic parameters at rest and during exercise were collected. Positive and negative groups were compared using Student’s t-test and Mann-Whitney U test.
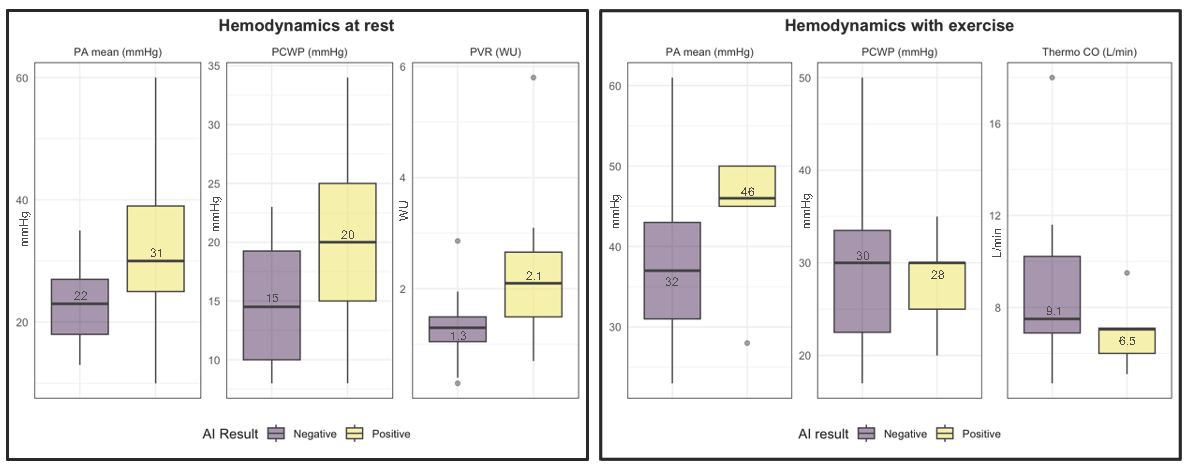
Results: A total of 47 patients (82% women, 79% Black, average EF 62%) had a previous RHC, with 23 undergoing subsequent exercise RHC. There were 18 patients (38%) with a positive AI result and 29 (62%) negative. Positive patients had significantly higher rates of atrial fibrillation (38% vs 11%, p=.03), NT-proBNP levels (median 451 vs 117 ug/mL, p=.001), and H2FPEF (median 6 vs 4, p<.001) and HFA-PEFF scores (median 5 vs 2, p=.005). Of 18 positive patients, 16 (89%) had a resting pulmonary capillary wedge pressure (PCWP) > 15 mmHg, consistent with HFpEF, compared to only 14 of 28 (50%) negative patients. With exercise 6 of 7 (86%) positive patients had PCWP ≥ 25 mmHg, consistent with HFpEF, compared to 11 of 20 (55%) negative patients. At rest, positive patients had significantly higher PCWP, mean pulmonary arterial pressure (mPAP), and pulmonary vascular resistance (PVR). After exercise, there were no significant differences in PCWP or mPAP between the two groups, but thermodilution cardiac output was significantly lower in the positive patients.
Conclusion: Patients identified as HFpEF positive by a validated TTE-guided AI tool were more likely to have HFpEF confirmed invasively, indicating its potential for risk stratification. However, the negative predictive value for HFpEF confirmed by invasive hemodynamics was low in this population.
Sachar, Ryan
(
University of Chicago
, Chicago , Illinois , United States )
Latz, Maria
(
University of Chicago
, Chicago , Illinois , United States )
Blair, John
(
University of Washington
, Seattle , Washington , United States )
Allan, Tess
(
University of Chicago
, Chicago , Illinois , United States )
Kim, Gene
(
University of Chicago
, Chicago , Illinois , United States )
Grinstein, Jonathan
(
University of Chicago
, Chicago , Illinois , United States )
Woodward, Gary
(
Ultromics
, Oxford , United Kingdom )
Lang, Roberto
(
University of Chicago
, Chicago , Illinois , United States )
Belkin, Mark
(
University of Chicago
, Chicago , Illinois , United States )
Author Disclosures:
Ryan Sachar:DO NOT have relevant financial relationships
| Maria Latz:No Answer
| John Blair:No Answer
| Tess Allan:No Answer
| Gene Kim:DO have relevant financial relationships
;
Consultant:Ctyokinetics:Active (exists now)
| Jonathan Grinstein:No Answer
| gary woodward:No Answer
| Roberto Lang:DO NOT have relevant financial relationships
| Mark Belkin:DO NOT have relevant financial relationships