Cardiac outcomes with different types of Heart Failure in Polycythemia vera: Analysis from National Inpatient Sample
Abstract Body (Do not enter title and authors here): Background Previous studies have shown poor outcomes in Polycythemia vera (PV) patients (pts) with comorbid heart failure (HF). Given lack of data, we studied the role of systolic heart failure (SHF), and diastolic heart failure (DHF), with and without acute exacerbation in PV pts from a national database.
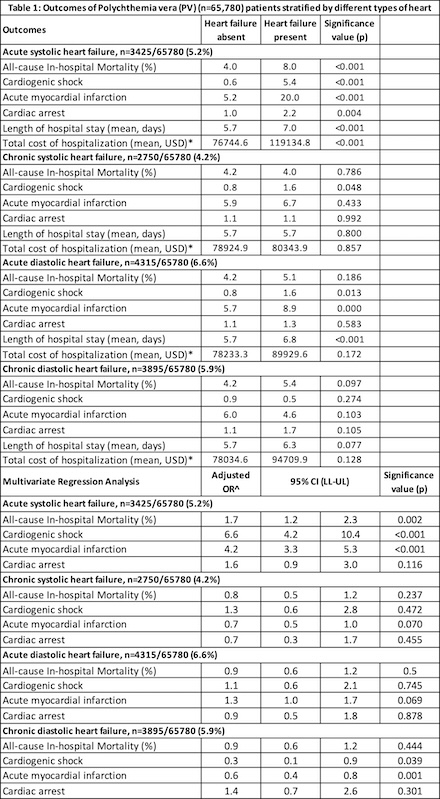
Methods Using National Inpatient Sample 2019-21, we identified all pts with PV. They were further reclassified into 4 different study populations depending on type of HF. This included MM pts with and without acute SHF, chronic SHF, acute DHF, and chronic DHF. In each study population, we excluded those with any other type of comorbid HF. Outcomes were compared using Pearson’s chi-square test and multivariate regression analysis.
Results 65780 had PV. Among them 5.2% (n=3425) had only acute SHF, 4.2% (n=2750) had chronic SHF, 6.6% (n=4315) had acute DHF, and 5.9% (n=3895) had chronic DHF. Those with acute SHF had significantly higher odds of mortality (adjusted odds ratio (aOR) 1.7, p=0.002), cardiogenic shock (CS) (aOR 6.6, p<0.001), acute myocardial infarction (MI) (aOR 4.2, p<0.001), and similar odds of cardiac arrest (CA) (aOR 1.6, p=0.116). Those with chronic SHF had similar odds of mortality (aOR 0.8, p=0.237), CS (aOR 1.3, p=0.472), acute MI (aOR 0.7, p=0.07) and CA (aOR 0.7, p=0.455). Similarly, those with acute DHF had similar odds of mortality (aOR 0.9, p=0.5), CS (aOR 1.1, p=0.745), acute MI (aOR 1.3, p=0.069) and CA (aOR 0.9, p=0.878). Those with chronic DHF also had similar odds of mortality (aOR 0.9, p=0.444), and CA (aOR 1.4, p=0.301), and lower odds of CS (aOR 0.3, p=0.039), and acute MI (aOR 0.6, p=0.001). Please refer Table 1 for rates of complication (Pearson’s chi-square).
Conclusion Among different types of HF in PV pts, acute SHF is associated with higher odds of mortality and even significantly higher odds of cardiac complication like CS (560%), acute MI (320%). All other types of HF including chronic SHF, acute DHF and chronic DHF showed similar odds of mortality and similar or even lower (for chronic DHF) odds of cardiac complications. This data helps guide timing for cardiology consultation and need for care escalation depending on HF type in PV.
Modi, Karnav
(
University of Missouri - Kansas City
, Kansas City , Missouri , United States )
Mahadevia, Himil
(
University of Missouri - Kansas City
, Kansas City , Missouri , United States )
Modi, Ronak
(
SMIMER Hospital & Medical College
, Surat , Gujarat , India )
Bavishi, Shriya
(
University of Connecticut
, Hartford , Connecticut , United States )
Vodnala, Deepthi
(
SLCC
, Kansas City , Missouri , United States )
Khumri, Taiyeb
(
SLCC
, Kansas City , Missouri , United States )
Asif, Talal
(
University Health Truman Medical Center
, Kansas City , Missouri , United States )
Author Disclosures:
Karnav Modi:DO NOT have relevant financial relationships
| Himil Mahadevia:DO NOT have relevant financial relationships
| Ronak Modi:No Answer
| Shriya Bavishi:DO NOT have relevant financial relationships
| Deepthi Vodnala:No Answer
| Taiyeb Khumri:DO NOT have relevant financial relationships
| TALAL ASIF:DO NOT have relevant financial relationships