Benefits and Risks Associated with Mineralocorticoid Receptor Antagonists in Tafamidis-treated Transthyretin Amyloid Cardiomyopathy: A Real-World Analysis
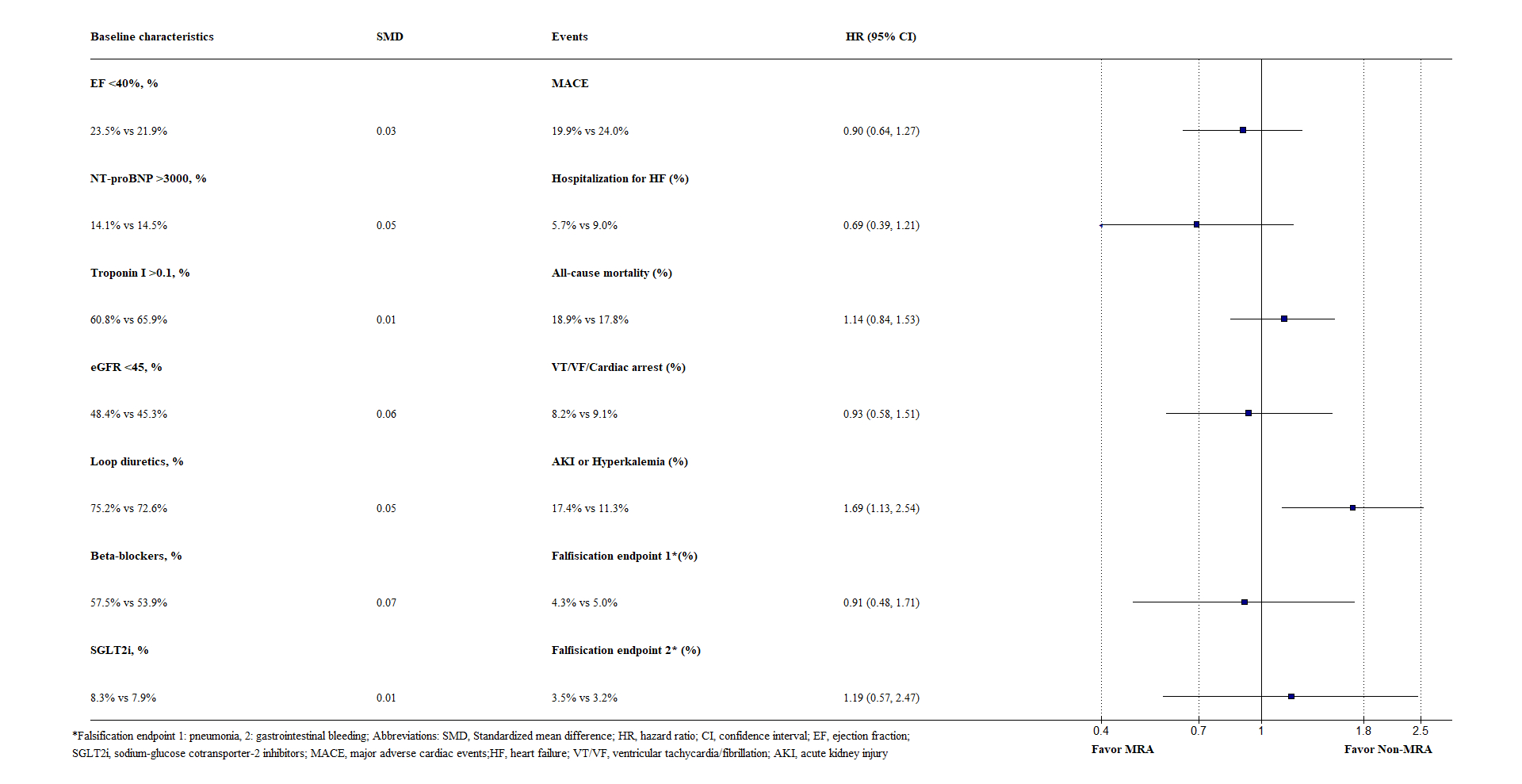
Abstract Body (Do not enter title and authors here): Background There is currently no data on the use of mineralocorticoid receptor antagonists (MRA) in tafamidis-treated transthyretin amyloid cardiomyopathy (ATTR-CM). Research Question Does the addition of MRA provide extra benefits in ATTR-CM patients treated with tafamidis? Aim To assess the benefits and risks associated with MRA in tafamidis-treated ATTR-CM through a new-user design propensity-score matching (PSM) analysis. Methods We conducted a retrospective, PSM cohort study using the TriNetX Global database. We included adult ATTR-CM patients who had their first tafamidis prescription within 1 year after the identification of amyloidosis between January 1, 2018, and May 1, 2023. MRA users and non-users were subsequently identified, with the former defined as those having both tafamidis and spironolactone/eplerenone, and the latter having tafamidis without MRA. Patients with prior MRA use before their first tafamidis prescription were excluded. The primary endpoint was major adverse cardiac events (MACE), defined as a composite of all-cause mortality, heart failure (HF) hospitalization, or cardiac arrest/ventricular tachycardia/fibrillation. Secondary endpoints were individual MACE. The safety endpoint was a composite of acute kidney injury (AKI) or hyperkalemia. Incident gastrointestinal bleeding and pneumonia were set as falsification endpoints. We compare study endpoints occurring within two years of tafamidis initiation between MRA users and non-users. Results Among 2,174 tafamidis-treated ATTR-CM patients, 471 MRA users were matched to 471 non-users with similar age (76.7 vs. 76.7), sex (female, 16.8% vs. 17.4%), and mean ejection fraction (50.1% vs. 49.9%). Amyloid staging markers and important medications were also balanced (Figure). MRA use was not associated with a significant reduction in MACE (HR, 0.90; 95% CI, 0.64 to 1.27) (Figure). Conversely, it was associated with a significant increase in AKI or hyperkalemia (HR, 1.69; 95% CI, 1.13 to 2.54) (Figure). The two falsification endpoints were comparable between the two groups (Figure). Conclusions In ATTR-CM patients treated with tafamidis, MRA was not associated with a significant reduction in MACE but with an increased risk of AKI or hyperkalemia.
Chi, Kuan Yu
(
Jacobi Medical Center, Albert Einstein College of Medicine
, Bronx , New York , United States )
Borkowski, Pawel
(
Jacobi Medical Center
, Bronx , New York , United States )
Osabutey, Anita
(
Jacobi Medical Center, Albert Einstein College of Medicine
, Bronx , New York , United States )
Varrias, Dimitrios
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Song, Junmin
(
Jacobi Medical Center
, Bronx , New York , United States )
Chang, Yu
(
National Cheng Kung University Hospital
, Tainan , Taiwan )
Madan, Shivank
(
Montefiore Medical Center, Albert Einstein College of Medicine
, Bronx , New York , United States )
Patel, Snehal
(
Montefiore Medical Center, Albert Einstein College of Medicine
, Bronx , New York , United States )
Author Disclosures:
Kuan Yu Chi:DO NOT have relevant financial relationships
| Pawel Borkowski:DO NOT have relevant financial relationships
| Anita Osabutey:DO NOT have relevant financial relationships
| Dimitrios Varrias:No Answer
| Junmin Song:DO NOT have relevant financial relationships
| Yu Chang:No Answer
| Shivank Madan:No Answer
| Snehal Patel:No Answer